To diagnose whooping cough in modern times, a large number of tests and analyzes are available, but how to choose the right and most accurate one?
So, many experts around the world recommend:
If the cough in adolescents and adults lasts less than two weeks, and in children less than three weeks, then it is advisable to use microbiological methods (culture) or amplification diagnostic methods (polymerase chain reaction, PCR) [1,2].
If a cough in children and adults lasts more than two weeks and no vaccination against whooping cough has been carried out during the current year, then it is advisable to use serological diagnostic methods (for example, enzyme-linked immunosorbent assay, ELISA) [1,2].
Now a little more about the important features of each method.
Polymerase chain reaction (PCR).
The required material for analysis is a nasopharyngeal smear, but it is preferable to use a nasopharyngeal mucus sample [3].
PCR must be carried out within the first two to three weeks from the onset of cough, since after four weeks from the onset of the disease, the number of B. pertussis bacteria in the nasopharyngeal secretion rapidly decreases, and the number of bacteria also decreases if antibacterial therapy was carried out (more than 5 days [4]) .
In infants and previously unvaccinated children, PCR can be performed within the first four weeks from the onset of cough [4,5].
For greater accuracy, PCR is always recommended to be carried out in parallel with culture [1], therefore, when collecting material, two samples should be taken at the same time - one for PCR, the other for culture. For what? PCR can give false-positive results, since it only determines the presence or absence of pathogen DNA, and not the presence of living forms [6].
When collecting PCR, it is recommended to use sticks made of nylon, rayon and polyester. When using cotton wool, the pathogen dies [7].
When pertussis is suspected, it is important to carry out differential diagnosis with adenovirus, bocavirus infections, influenza, parainfluenza, M. pneumoniae, Chlamydia trachomatis and Chlamydia pneumoniae [8].
PCR is not recommended for persons who have been in contact with a patient with whooping cough in the absence of any symptoms [7].
Sowing.
Culture on a nutrient medium is the gold standard for diagnosing whooping cough [1–4].
A high probability of obtaining the most accurate result is observed in people who have had a cough for less than two weeks, if antibacterial drugs have not yet been used for treatment and if vaccination against whooping cough was carried out more than 12 months ago [4].
The material required for culture is nasopharyngeal discharge.
The causative agent of whooping cough - B. pertussis is a very sensitive and fastidious microorganism, therefore it is recommended that medical personnel strictly follow the instructions and observe the technique of collecting material for analysis.
On average, the culture result can be ready in 4-10-14 days [9,10], it all depends on the capabilities of the laboratory. In those who have not previously been ill and have not been vaccinated against whooping cough, the preliminary culture result can be ready within 72-96 hours [9,11].
The great advantage of culture is that it is possible to determine the sensitivity of a microorganism to antibiotics and, therefore, to correctly select drugs for subsequent treatment. In addition, according to culture data, it is possible to determine which specific strain of bacteria is circulating in a certain area and evaluate the effectiveness of the vaccine used [12].
Etiology of whooping cough
Whooping cough is an acute airborne infection caused by microorganisms of the species Bordetella pertussis, characterized by damage to the mucous membrane mainly of the larynx, trachea, bronchi and the development of convulsive paroxysmal cough.
The bacteria that cause whooping cough were first isolated from a sick child in 1906 by two scientists - the Belgian Jules Bordet (the genus is named after him) and the Frenchman Octave Zhangou (in honor of both of them, the causative agent of whooping cough is also called the Bordet-Gengou bacillus). In addition to describing the microbe, they developed a nutrient medium for its cultivation, which is widely used to this day and is also called Bordet-Gengou medium in their honor.
In modern taxonomy, Bordetella belongs to the domain Bacteria, order Burcholderiales, family Alcoligenaceae, genus Bordetella. Within the genus, 9 species are described, 3 of which are predominantly pathogenic for humans:
- most often the disease is caused by B. pertussis, the causative agent of whooping cough, an obligate human pathogen;
- B. parapertussis is the causative agent of parapertussis (whooping cough-like disease, clinically similar to whooping cough), also isolated from some animals;
- B. trematum is a causative agent of wound and ear infections, described relatively recently.
There are 4 more species that are causative agents of animal diseases, but are also potentially pathogenic for humans (they cause infections in especially rare cases, usually in immunocompromised patients):
- B. bronchiseptica is the causative agent of bronchisepticosis (whooping cough-like disease of animals, in humans it occurs as an acute respiratory infection);
- B. ansorpii, B. avium, B. hinzii. B. holmesii is isolated only from humans, usually during invasive infections (meningitis, endocarditis, bacteremia, etc.), but the etiological role of this species in the development of infections has not been proven.
- B. petrii is the only representative of the genus isolated from the environment and capable of living in anaerobic conditions, but the possibility of its long-term persistence in humans has been described.
Previously, until the 30s of the last century, Bordetella was erroneously assigned to the genus Haemophilus only on the grounds that it was necessary to add human blood to the media for their cultivation.
Most media are still filled with defibrinated human blood. However, Breadford in later studies showed that blood is not a growth factor for Bordetella and an essential component during cultivation, but plays more of an adsorbent role for toxic metabolic products of bacteria.
In terms of genotype and phenotypic properties, Bordetella also differ significantly from Hemophilus, which was proven by Lopes in the 50s of the 20th century. This made it possible to distinguish them into an independent genus.
Enzyme-linked immunosorbent assay (ELISA).
In case of late diagnosis, when the cough lasts more than 3-4 weeks and/or antibiotic therapy has already been started or carried out, serological diagnostic methods, for example, enzyme-linked immunosorbent assay (ELISA), can be used to confirm whooping cough in laboratory.
Using ELISA, you can detect antibodies of the IgM, IgA and IgG classes to various pathogen antigens: pertussis toxin (PT), filamentous hemagglutinin (FHA), pertactin (PRN). The most specific antigen is pertussis toxin, since it is the only antigen that is characteristic only of B. pertussis [12]. Other antigens may also be present in other representatives of Bordetella.
Antibodies to pertussis toxin may be absent in 25% of infants and 10% of adolescents [2,3].
Serological testing for the diagnosis of whooping cough can be used from 3 to 12 weeks after the onset of cough [13,14]. The material for research is blood.
Laboratory diagnosis of whooping cough and recommended time intervals for performing various tests
Which class of antibodies is best to determine?
1. Antibodies of the IgM .
- Indicate an acute infectious process.
- They are formed no earlier than the second week from the onset of the disease, therefore, their determination before this period is impractical [9,14].
- In some children and adults, regardless of vaccination or previous illness, IgM antibodies may be produced in small quantities and not determined by analysis [9].
- If IgM determination was carried out in the first two weeks from the onset of the disease and the result was negative, then it is recommended to repeat the test after 10-14 days. If a negative result is obtained 14 days after the onset of the disease, then there is no point in redoing the analysis, since over time the amount of IgM only decreases.
IgG class antibodies .
- They are detected in the third week from the onset of the disease, reach their highest value at 6-8 weeks of illness, after which their level gradually decreases [9].
Determination of specific IgG is the most common and standardized method for the serological diagnosis of whooping cough [2,3]
- For more accurate diagnostics when determining IgG, it is recommended to use paired sera, since it is difficult to draw a reliable conclusion from the data of one analysis, because it is not known what the presence of IgG is associated with - a disease or a previous vaccination.
- The recommended interval between studies is 10-14 days. The result is considered positive when the titer increases by 2-4 times or more [3,9,15].
Antibody titer determination is the optimal method for diagnosing pertussis in previously immunized adolescents and adults [1,9].
IgG testing is recommended if no pertussis vaccination has been performed within the current year (12 months) [1,9].
- When examining a single serum sample (even from an adult or child previously vaccinated more than 12 months ago), the result of detecting IgG antibodies can be regarded as positive only in the case of a high titer (the exact value must be clarified in the laboratory, since data vary depending on the technique analysis and reagents used) [14].
In the “Additional materials” tab below you can download a memo about the features of laboratory diagnostics of whooping cough in pdf format.
Classic symptoms of the disease
If the symptoms of the disease are clear and treatment brings quick relief, blood is not taken for analysis, since there is no reason to suspect complications of the disease or an incorrect diagnosis.
Symptoms of the disease are:
temperature increase to more than 38 degrees;
attacks of cough that impair breathing, which cannot be confused with another cough (even if a person has encountered whooping cough for the first time, he will understand that the cough is atypical and will be able to make a diagnosis.
Attacks of convulsive cough occur in a series of coughing impulses, then a whistling deep breath and again short and convulsive impulses. There can be 2 to 15 such “cycles” in an attack. At the end of the attack, glassy sputum is released, and sometimes vomiting occurs.
protruding tongue when coughing in children, the face is bluish, the veins in the neck are swollen, suffocation may occur
nausea, even vomiting after a coughing attack;
sleep disturbance due to coughing attacks, which can be from 5 to 50 per day.
Often, when a child coughs, he injures his protruding tongue, and wounds appear on it, which is typical only for whooping cough. Sometimes there may also be tears in the corners of the mouth and on the frenulum of the lower lip. In adults, traumatic symptoms are absent due to the strength of the tissues and greater ability to control one’s behavior during an attack.
Infection from a patient is possible from the first day of illness. Most often it occurs through direct contact and less often through household objects, since the pathogen is unstable in the external environment. Outbreaks of whooping cough occur primarily in children's institutions. People get sick with whooping cough only once, since a strong immune system resists its pathogen well throughout their life. In adults, due to the large width of the trachea, there are no attacks of suffocation, the disease is mild and the patient does not see the need to see a doctor.
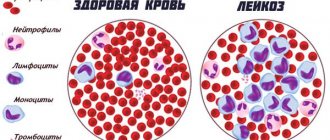
Clinical blood test.
A general blood test for whooping cough is characterized by an increase in the number of leukocytes and lymphocytes [1-4]. The number of lymphocytes increases under the influence of the pertussis toxin. [2], however, the absence of an increase in leukocytes does not exclude whooping cough. A clinical blood test is only an additional diagnostic method [5].
There is evidence that if, according to the results of a clinical blood test, a child has more than 10,000 leukocytes in 1 μl and more than 50% of them are lymphocytes, then the diagnosis of whooping cough can be considered probable (of course, in the presence of a characteristic clinical picture) [16]. If in a repeated analysis - after 24 hours - there is an increase in leukocytes of more than 20,000 in 1 μl and of these more than 50% are lymphocytes, then this indicates that the probability of whooping cough is extremely high [16].
When assessing a clinical (general) blood test in young children, it should also be remembered that if during pregnancy the baby’s mother was vaccinated against whooping cough, then there may not be an increase in leukocytes [16].
How and where to submit
Each analysis has its own procedure for collecting material:
- For CBC, capillary and venous blood is taken from the child;
- ELISA is carried out on the basis of venous;
- When conducting bacterial culture and PCR, discharge from the nose and throat is used.
Research is carried out in private and public laboratories as prescribed by a doctor.
Clinic Hemotest
The medical laboratory Gemotest, whose centers are located in 65 cities of Russia, performs various tests aimed at detecting whooping cough. There are several types of research being conducted here.
| Name | Price, rub |
| Clinical analysis, including leukemia formula, ESR | 670 |
| Sowing | 1.000 |
| IgG | 820 |
| IgA | 830 |
| IgM | 820 |
| Sputum examination | 440 |
Price in Invitro
A number of tests to detect the bacteria that cause whooping cough can be taken at Invitro clinics located in many localities in Russia. Current prices are shown in the table:
| Name | Price, rub |
| CBC, including leukocyte count, ESR, manual smear analysis | 1.020 |
| KBC, including leukocyte formula, ESR | 720 |
| Bakposev | 1.415 |
| IgG | 825 |
| IgA | 825 |
| IgM | 825 |
There is an additional charge of 199 rubles. for drawing blood from a vein.