- June 22, 2018
- Oncology
- Katya Tkach
Recently, diseases associated with oncology have become more frequent, which bring people a lot of inconvenience and pain. Some of them are incurable and fatal, others are amenable to therapeutic adjustment and are practically not dangerous to life and health.
The second type of disease includes lymphogranulomatosis, the effective treatment of which was discovered back in the 1970s. What happens in the human body during this disease? What are the symptoms of lymphogranulomatosis and blood test indicators in adults? What are the methods to combat the disease? These issues are covered in the article.
Lymphogranulomatosis - what is it? Clinic and treatment
Lymphogranulomatosis (the second name is Hodgkin's lymphoma) - refers to a number of oncological diseases and is characterized as a disease of the lymphatic system, during which Berezovsky-Sternberg-Reed cells (the scientists who discovered this disease) can be detected in the lymphatic tissue.
The disease is diagnosed in children and adults. Lymphogranulomatosis is more common in adolescent children, and also occurs in adults aged 20, 50 years.
Results and forecast
The prognosis for Hodgkin's disease depends on timely diagnosis, the stage of the tumor process, the nature of the disease, and the presence of complications. After chemotherapy and radiotherapy, the percentage equivalent of patient survival for five years is:
- 90% – with local and regional stages of the disease;
- 80% – with generalized without intoxication by tumor decay products;
- 60% – with generalized with the presence of intoxication;
- 45% – at the disseminated stage.
Lymphogranulomatosis is a malignant pathology of lymphatic tissue that can metastasize throughout almost the entire body. General clinical and biochemical analysis determines the signs of the disease, but these results are not the basis for making a final diagnosis. Hodgkin's disease can only be diagnosed through an extensive examination of the patient.
Causes
Until the recent past, lymphogranulomatosis was considered a disease of infectious origin. It was believed that its causative agent could be the tuberculosis bacillus. Less commonly, this role was assigned to streptococcus, Escherichia coli, spirochete pallidum, and diphtheria bacillus. There were also suggestions about the viral etiology of lymphogranulomatosis, but this was also not confirmed.
It has now been established that tumor neoplasms (hematosarcomas and leukemias) are considered a certain pathology of the hematopoietic system, and malignant Berezovsky-Sternberg cells are the cause of the development of lymphogranulomatosis.
Also, certain life factors that may contribute to the onset of the disease are not fully understood. These include lifestyle, bad habits, diet and occupational hazards. Some studies provide data on the possible risk of lymphogranulomatosis in people who have had infectious mononucleosis or skin diseases, working in the clothing or woodworking industries, in agriculture, as well as among chemists and doctors.
Cases of lymphogranulomatosis have been reported among several members in one family or in one team. This suggests the existence of a role for a weakly virulent infection of viral etiology and the genetic predisposition of the body, however, there is no definitive evidence for this yet. Thus, specific and exact causes of lymphogranulomatosis have not yet been found.
General blood analysis
When conducting a general clinical analysis, capillary blood (from a finger) is most often used. During the study, the following deviations of the main blood parameters in adults with Hodgkin's disease are determined (relative to reference values)
| Indicators | Norm | Changes | |||
| men | women | ||||
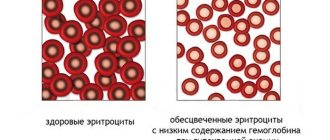
| blood cells (erythrocytes) | 4–5.1 g/l | 3.7–4.7 g/l | decline | ||
| hemoglobin | 130–160 g/l | 120–140 g/l | drop due to a decrease in the number of red blood cells | ||
| erythrocyte sedimentation rate (ESR) | 1–10 | 2–15 | increase to 30 due to connection (clumping) of red blood cells | ||
| lymphocytes | 18–40% | 18–40% | a sharp decline | ||
| monocytes | 2–9% | 2–9% | increase (promote granuloma formation) | ||
| neutrophils (band/segmented) | 1–6 /47–72 | 1–6/47-72 | increase in the third and fourth stages of the disease | ||
| eosinophils | 0–5% | 0–5% | increase proportional to tumor growth | ||
| platelets | 180–320 | 180–320 | decrease during the development of the disease | ||
| basophils | 0–1% | 0–1% | more than 1.2% | ||
Changes in the blood test are interpreted as a shift in the leukocyte formula:
- Eosinophilia. It is caused by the mobilization of eosinophils as the main neutralizers of foreign cells (in case of LGM - oncological ones).
- Absolute monocytosis. The surge in monocytes is explained by the body’s desire to get rid of the resulting granuloma.
- Thrombocytopenia. Malignant cells displace hematopoietic tissue, causing platelets responsible for blood clotting to die.
- Basophilia. The growth of basophils is caused by their ability to support inflammatory and oncological processes in the body.
The total number of leukocytes (more than 4.0 x 10 9 /l) is recorded already at the initial stage of the disease. A decrease in hemoglobin in the blood, a decrease in the number of red blood cells (hemolytic anemia, otherwise anemia) is a characteristic sign of oncohematological diseases. When treating lymphogranulomatosis, anemia may develop due to the chemotherapy used.
Measuring hematocrit (the proportion of cellular elements in the total volume of blood) and color index does not play a significant role in lymphogranulomatosis. These values are assessed to diagnose complications associated with Hodgkin's disease.
Pathological anatomy
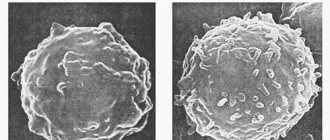
The detection of giant Reed-Berezovsky-Sternberg cells and their mononuclear precursors, Hodgkin cells, in a biopsy specimen is a mandatory criterion for the diagnosis of lymphogranulomatosis. According to many authors, only these cells are tumor cells.
All other cells and fibrosis are a reflection of the body's immune response to tumor growth. The main cells of lymphogranulomatous tissue, as a rule, will be small, mature T-lymphocytes of the CD2, CD3, CD4 > CD8, CD5 phenotype with varying numbers of B-lymphocytes. Histiocytes, eosinophils, neutrophils, plasma cells, and fibrosis are present to varying degrees.
Accordingly, there are 4 main histological types:
- The variant with nodular sclerosis is the most common form, accounting for 40-50% of all cases. It usually occurs in young women, is often located in the mediastinal lymph nodes and has a good prognosis. It is characterized by fibrous cords that divide the lymphoid tissue into “nodes”. It has two main features: Reed-Berezovsky-Sternberg cells and lacunar cells. Lacunar cells are large in size, have many nuclei or one multilobed nucleus, their cytoplasm is wide, light, foamy.
- The lymphohistiocytic variant accounts for approximately 15% of Hodgkin lymphoma cases. Men under 35 years of age are more often affected, it is detected in the early stages and has a good prognosis. Mature lymphocytes predominate, Reed-Berezovsky-Sternberg cells are rare. Low grade variant.
- The variant with suppression of lymphoid tissue is the rarest, less than 5% of cases. Clinically corresponds to stage IV of the disease. More common in elderly patients. Complete absence of lymphocytes in the biopsy specimen; Reed-Berezovsky-Sternberg cells predominate in the form of layers or fibrous cords or a combination thereof.
- The mixed cell variant accounts for approximately 30% of cases of Hodgkin lymphoma. The most common variant in developing countries, in children and the elderly. Men are more often affected; clinically it corresponds to stages II-III of the disease with typical general symptoms and a tendency to generalize the process. The microscopic picture is characterized by great polymorphism with many Reed-Berezovsky-Sternberg cells, lymphocytes, plasma cells, eosinophils, and fibroblasts.
The incidence of the disease is approximately 1/25,000 people/year, which is about 1% of the rate for all malignant neoplasms in the world and approximately 30% of all malignant lymphomas.
Leukocytes. What is this?
The very first thing that should interest you in the results of a blood test for lymphogranulomatosis is the leukocyte count.
Leukocytes are a group of blood cells of various shapes and functions, the main activity of which is to protect the body and strengthen the immune system. These white blood cells also perform a vital function against cancer. They are able to penetrate into the intercellular space to absorb and digest foreign particles, including tumor cells.
Among other indicators of a blood test for lymphogranulomatosis (the symptoms of which were described above), the coefficients of basophils, neutrophils, eosinophils, lymphocytes and monocytes are distinguished. These are different types of leukocytes, different in structure and function. Let's talk about them in more detail.
Basophils are endowed with the ability to migrate from the blood to the tissues. In the process of cell destruction, they release necessary substances into the surrounding tissues, thereby participating in the development of inflammatory and allergic reactions in the body.
Neutrophils absorb and destroy foreign bodies, and also produce antibacterial particles and substances that relieve intoxication.
Eosinophils penetrate the site of inflammation and produce special antibodies to completely destroy foreign cells (cancerous, toxic or parasitic).
Lymphocytes direct the protective activity of all leukocytes, and also produce the necessary antibodies in order to provide a double resistance to foreign bodies during re-infection.
Monocytes are capable of eliminating not only foreign particles, but also their own leukocytes that died during inflammation. If the foreign body cannot be destroyed, monocytes surround it, thereby preventing the spread of the harmful process.
What is the norm for the presence of leukocytes in the blood and what indicators will help determine the disease? Let's find out about this further.
Symptoms
The first symptoms that a person notices are enlarged lymph nodes. The onset of the disease is characterized by the appearance of enlarged dense formations under the skin. They are painless to the touch and may occasionally decrease in size, but subsequently increase again. Significant enlargement and soreness in the area of the lymph nodes is observed after drinking alcohol.
In some cases, enlargement of several groups of regional lymph nodes is possible:
- Cervical and supraclavicular – 60-80% of cases;
- Mediastinal lymph nodes – 50%.
Along with local symptoms, the patient is seriously concerned about general manifestations (group B symptoms):
- Excessive sweating at night (see causes of excessive sweating in women and men);
- Uncontrolled weight loss (more than 10% of body weight within 6 months);
- Fever that persists for more than one week.
Clinic “B” characterizes a more severe course of the disease and allows one to determine the need for intensive care.
Other symptoms characteristic of lymphogranulomatosis include:
- Skin itching;
- Ascites;
- Weakness, loss of strength, loss of appetite;
- Bone pain;
- Cough, chest pain, difficulty breathing;
- Abdominal pain, indigestion.
In some cases, the only symptom of lymphogranulomatosis for a long time is only a constant feeling of fatigue.
Breathing problems occur when the intrathoracic lymph nodes become enlarged. As the nodes grow, they gradually compress the trachea and cause constant coughing and other breathing problems. These symptoms are worse when lying down. In some cases, patients note pain behind the sternum.
How to recognize chronic diseases?
Symptoms of Hodgkin's lymphoma
In chronic Hodgkin's lymphoma, symptoms develop slowly and unnoticed. Hodgkin's disease can be recognized by the following signs:
- An increase in the size of one lymph node (inguinal, cervical, submandibular). The enlargement is small, the lymph node itself is small, dense and does not cause pain. After some time, it may completely disappear and appear again.
- Tumor cells of Hodgkin lymphoma are concentrated in nearby lymph nodes. As a result, they also enlarge and resemble sacks of potatoes.
- Fatigue, poor sleep and appetite.
- Headache.
- Increase in body temperature.
The chronic course of Hodgkin's lymphoma can occur completely unnoticed. In this case, the patient’s general condition is not disturbed at all, and he can carry out all his usual activities.
Stages of the disease with lymphogranulomatosis
Clinical manifestations of granulomatosis increase gradually and pass in 4 stages (depending on the prevalence of the process and the severity of symptoms).
Stage 1 - the tumor is in the lymph nodes of one area (I) or in one organ outside the lymph nodes.
Stage 2 - involvement of lymph nodes in two or more areas on one side of the diaphragm (top, bottom) (II) or an organ and lymph nodes on one side of the diaphragm (IIE).
Stage 3 - damage to the lymph nodes on both sides of the diaphragm (III), accompanied or not by organ damage (IIIE), or damage to the spleen (IIIS), or all together.
- Stage III(1) - the tumor process is localized in the upper part of the abdominal cavity.
- Stage III(2) - damage to the lymph nodes located in the pelvic cavity and along the aorta.
Stage 4 - the disease spreads in addition to the lymph nodes to internal organs: liver, kidneys, intestines, bone marrow, etc. with their diffuse damage
To clarify the location, use the letters E, S and X, their meaning is given below. Each stage is divided into category A and B according to the following.
Letter A - the patient has no symptoms of the disease
Letter B—presence of one or more of the following:
- unexplained loss of body weight more than 10% of the initial weight in the last 6 months,
- unexplained fever (t > 38 °C),
- drenching sweats.
Letter E - the tumor spreads to organs and tissues located next to the affected groups of large lymph nodes.
The letter S is a lesion of the spleen.
The letter X is a large volumetric formation.
Signs of the disease: enlarged lymph nodes
At the initial stage, no one can diagnose lymphogranulomatosis. Symptoms in adults and children do not provide a clinical picture of the disease. Sometimes this happens by chance during an ultrasound examination of the lungs, in which case enlarged structures of the nodes will be visible on the image. Only in the later stages, with obvious manifestations of pathology, is a conclusion about the disease made.
Manifestations of Hodgkin's disease:
- Enlarged lymph nodes.
- Systemic manifestations of the disease.
- Damage to internal organs and severe symptoms of disruptions in their functionality.
The first and constant sign of the disease is an enlargement of one or more lymph nodes. The manifestation can occur anywhere - in the armpit, neck, groin. The patient does not experience any discomfort - there is no fever, general health is normal. When palpated, the nodes do not cause pain; they roll under the skin, resembling a dense ball that gradually increases in size.
Diagnostics
To identify malignant granuloma, the most modern methods of laboratory and instrumental examination are used today. Founded:
- on detailed blood tests;
- highly specific monitoring tests for the level of tumor markers;
- PET studies;
- MRI examination of the organs of the peritoneum, chest and neck;
- radiography;
- Ultrasound examination of the lymph nodes of the peritoneum and pelvic region.
The morphological status of the tumor is determined by punctuation of the lymph nodes, or by the method of complete removal of the node to identify binucleate large cells (Reed-Berezovsky-Sternberg). Using bone marrow examination (after a biopsy), a differentiated diagnosis is carried out, excluding other malignant neoplasms.
It is possible to prescribe cytogenetic and molecular genetic tests. [adsen]
Distribution mechanism
The basic differences between lymphogranulomatosis and other types of lymphomas are as follows:
- The presence of binucleate giant Reed-Sternberg cells in the nodes.
- The presence of mononuclear large Hodgkin cells.
- The inclusion of a large number of blood cells (erythrocytes, leukocytes, eosinophils, plasma cells, etc.) in the lymphoma.
There is one more characteristic feature that defines lymphogranulomatosis. Symptoms appear when the first lymph node is affected (on the neck, in the subclavian region, in the mediastinum), and metastases spread through the lymphatic and blood vessels, growing into organs adjacent to the lesions - lungs, gastrointestinal tract, bone marrow, kidneys, etc.
How to treat lymphogranulomatosis?
The main method of treating patients with lymphogranulomatosis is combined chemoradiotherapy, which varies in intensity depending on the volume of the tumor mass, that is, the total number of tumor cells in all affected organs.
In addition, the following factors influence the prognosis:
- massive lesion of the mediastinum;
- diffuse infiltration and enlargement of the spleen or the presence of more than 5 foci in it;
- tissue damage outside the lymph nodes;
- damage to lymph nodes in three or more areas;
- an increase in ESR more than 50 mm/h in stage A and more than 30 mm/h in stage B.
To treat patients with an initially favorable prognosis, 2 to 4 courses of chemotherapy are used in combination with irradiation of only the affected lymph nodes. In the group with an intermediate prognosis, 4-6 cycles of polychemotherapy and irradiation of the affected areas of the lymph nodes are used. In patients with an unfavorable prognosis of the disease, 8 courses of polychemotherapy and irradiation of areas with a large array of affected lymph nodes are carried out.
When is lymphogranulomatosis diagnosed?
Lymphogranulomatosis (LGM) or malignant granuloma is a type of lymphoma, a cancer of the lymphatic system. Lymphoma develops when cells in lymph nodes begin to grow out of control and compress nearby tissue or spread throughout the body through the lymphatic circulation. LGM differs from other types of lymphomas in the nature of its growth and spread.
Lymphogranulomatosis in history
Another name for LGM is Hodgkin's disease. The pathology was named after Thomas Hodgkin, a British physician who first described abnormalities in the lymphatic system in 1832. However, Hodgkin noted that the earliest description of the disease may have been given by Marcello Malpighi in 1666.
While working at the hospital, Hodgkin studied seven patients whose lymph nodes were enlarged but not painful. One of these people was a patient of Robert Carswell, whose report included many of the illustrations used in early descriptions of the condition. Hodgkin wrote a report on seven patients, which was presented to the medical community in London in 1832.
In 1856, Samuel Wilkes reported an even larger number of patients with the same disease described by Hodgkin.
In 1872, Langhans described the features of Hodgkin's lymphoma at the microscopic level, and Carl Sternberg and Dorothy Reed first pointed out the cytogenic characteristics of cancer cells in 1898 and 1902, respectively. Today these cells are called Reed-Sternberg cells (RS cells).
Treatment for Hodgkin's lymphoma dates back to 1894, using Fowler's solution containing arsenic. In 1932, Chevalier and Bernard described the use of radiation therapy in treating the condition, primarily for palliative purposes (relief but not cure). Evidence of the effectiveness of radiation therapy was obtained in the mid-forties.
In 1963, a combination of chemotherapeutic agents was developed that consisted of cyclophosphamide, vincristine, methotrexate and prednisone. Another chemotherapy regimen was introduced in 1987 and included epirubicin, bleomycin, vinblastine, and prednisone.
In 1992, a German research group developed a chemotherapy regimen that used seven agents: bleomycin, etoposide, adriamycin, cyclophosphamide, Oncovin, procarbazine, and prednisone.
What organs and systems are affected?
LGM is a type of cancer that develops in the lymphatic system, which is part of the immune system.
Composition of the lymphatic system
- lymph. A colorless, watery fluid that transports lymphocytes through the lymphatic system. Lymphocytes are a type of white blood cell (leukocyte). There are 2 main types of lymphocytes: B lymphocytes (B cells): B cells produce antibodies to protect the body from bacteria and viruses. LGM usually begins with B lymphocytes;
- T lymphocytes (T cells): There are many types of T cells. Some T cells destroy germs or abnormal cells in the body. Other T cells promote or inhibit the activity of other cells of the defense system;
LGM most often spreads through lymphatic vessels from one lymph node to another. Rarely, late in the disease, it may invade the bloodstream and spread to other parts of the body (liver, lungs and/or bone marrow).
Pathophysiology
RS cells are cancer cells of LGM. This type of cells is considered a hallmark of LGM, although similar cells are observed in infectious mononucleosis and other types of lymphomas. The RS cell arises from the B cell germinal center. LGM, in which the RS cell is of T cell origin, is rare. LGM is characterized by a variable number of RH cells surrounded by an inflammatory infiltrate (accumulation) of lymphocytes, plasma cells and eosinophils in different proportions, depending on the histological subtype of LGM.
Forecast
The stage of the disease is of greatest importance in the prognosis for lymphogranulomatosis. Patients with stage 4 disease have a 75% five-year survival rate, while patients with stages 1-2 have a 95% survival rate. The prognosis for signs of intoxication is poor. Early signs of an unfavorable course of the disease are “biological” indicators of activity.
Biological indicators of activity include:
- alpha-2-globulin more than 10 g/l,
- haptoglobin more than 1.5 mg%,
- an increase in ESR in the general blood test of more than 30 mm/h,
- increase in fibrinogen concentration more than 5 g/l,
- cerruloplasmin more than 0.4 extinction units.
If at least 2 of these 5 indicators exceed the specified levels, then the biological activity of the process is determined.
Treatment
The following treatment methods are used in the treatment of malignant granuloma:
- radiotherapy - radiation exposure to the affected lymph nodes. 1 course of such therapy usually lasts 4-5 weeks. This method of treatment is effective at the initial stage of lymphogranulomatosis, but at stages 3 and 4 of the diagnosis, a combination of radiotherapy with radiation or chemotherapy is required;
- drug therapy. It consists of a combination of drugs that have an antitumor effect. 1 course of chemotherapy usually lasts 14-30 days. Patients with this disease are usually prescribed drugs that destroy damaged carcinogenic cells and stop their division. In some cases, it may be advisable to prescribe prednisolone, a hormonal drug that has an anti-inflammatory effect. Drug therapy is usually used in stages 3 and 4 of the disease in conjunction with radiotherapy;
- surgical removal of a cancerous tumor. It is used only in cases where other treatment methods are not effective enough. It is aimed at improving the patient's condition, but is not able to completely cure the disease.
The question “How long do people live with Hodgkin lymphoma” can often be given a favorable answer for the patient. With timely initiation of therapy, lymphogranulomatosis can lead to complete disappearance of the symptoms of the disease.
Prevention
Unfortunately, to date, effective prevention of this disease has not been developed. More attention is paid to the prevention of relapses; this requires strict adherence to the prescribed treatment program for lymphogranulomatosis and the implementation of the necessary regimen and rhythm of everyday life.
Among the most common reasons for the recurrence of the disease are insolation and pregnancy. After suffering from this disease, the possibility of pregnancy is possible two years after remission.
Advice for those suffering from illness
If you are diagnosed with LGM, it is important to remember how well you take care of your body during treatment. Following a healthy diet and exercising regularly as much as possible can potentially improve your overall well-being.
A healthy balanced diet should include:
- complex carbohydrates, including whole grains;
- easily digestible proteins;
- dairy products;
- lots of fruits and vegetables;
- healthy fats found in nuts, avocados and olive oil;
- sufficient amount of liquid.
Research has shown that staying active during LGM treatment can improve your physical endurance and your prognosis for recovery. In addition to building muscle and bone strength, regular exercise reduces anxiety and fatigue, improves heart function and improves self-esteem.