Medical history
The history of the disease of this type goes back to 1855, when the British doctor Addison gave a detailed explanation of this disease, and in 1872 the German doctor Birmer supplemented the description of this pathology, and after that the lack of vitamin B12 began to be characterized as anemia, which is malignant in nature.
At that time, there were no methods for correctly diagnosing the pathology, as well as qualified treatment, so hemoglobin dropped to 30.0 g/l and below, the person fell into a coma, which led to death.
Only in the 20th century in 1926, a discovery was made, which was appreciated by the Nobel proverb, that anemia with vitamin B12 deficiency is the inability of the stomach organ to produce a specific enzyme that helps the absorption of this vitamin from the digestive system.
Blood for B12 deficiency anemia
Decoding the results
So that you can roughly navigate the results, we present possible indicators: the norm of vitamin B12 in the blood of people of different ages and numbers indicating deviations.
Optimal performance
The level of vitamin B12 in the blood directly depends on age:
| Age (years) | Vitamin B12 norm (ng/l) |
| up to 1 | 292-1205 |
| 2-3 | 265-1214 |
| 3-6 | 246-1077 |
| 7-9 | 280-1172 |
| 10-12 | 183-1081 |
| 13-18 | 214-864 |
| adult women and men | 200-1000 |
There are indicators for ml of blood, but not all laboratories use them. It is easy to see that the spread between the smallest and largest numbers is quite wide. Gender does not affect the level of vitamin B12 in the blood; in adult men and women it can be the same.
Level too low
If, according to the results of the analyses, the numbers clearly do not reach those listed in the table above, this is a reason to look for the root cause. Vitamin B12 may be below normal for the following reasons:
- long-term veganism;
- eating disorders such as anorexia nervosa;
- fasting or low calorie diets;
- pancreatitis or other gastrointestinal problems;
- impaired absorption in the intestine;
- Zollinger-Ellison or Imerslund-Gresbeck syndromes;
- parasites in the intestines;
- blood cancer.
Sometimes the level of vitamin B12 in the blood can be low due to the genetic characteristics of the body. If the analysis shows a deficiency in an infant, then the mother also needs to be checked. The baby receives almost no useful substance from milk.
If the concentration of vitamin B12 in the blood is slightly below normal, this is a signal that you need to adjust your diet. It is enough to eat fish, meat, offal, liver and milk every day. If your vitamin B12 deficiency is severe, you should consult your doctor about taking supplements. After completing the course, you must be tested for vitamin B12 again.
Now Foods, Methyl B-12, 1000 mcg, 100 Lozenges
from 555 ₽
More details
Level too high
This situation is much less common, but it also has certain reasons:
- liver diseases;
- heart problems;
- blood cancer;
- renal failure;
- disturbances in the functioning of the small intestine.
Unlike deficiency, exceeding the norm of vitamin B 12 is not considered dangerous. If the numbers go off scale, this is a reason to be examined more thoroughly. B12 levels don’t just rise, it can indicate more serious diseases.
The vitamin content is not artificially reduced; it will balance itself over time. The main attention should be paid to diagnosed diseases, and the entire body must be examined. An excess of cobalamin signals possible diseases in almost all organs and systems. Later, it is advisable to take a vitamin B 12 test again to check the dynamics.
Megaloblastic type of anemia
Pernicious (with B12 deficiency) anemia refers to the megaloblastic form of anemia, and is quite rarely combined with another megaloblastic folate deficiency anemia.
Megaloblastic anemia is a fairly rare form of pathology in which there is a deviation from the normal absorption of the digestive system of folic acid, vitamin B12 and the substance cyanocobalamin.
As a result, there is a lack of B vitamins in the body: B12 and B9.
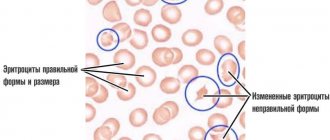
Megaloblasts are modified red blood cells that are synthesized in DNA and RNA cells. Megaloblasts appear in bone marrow cells as a consequence of a deviation in the synthesis procedure. This is manifested in morphological changes in the composition of cells.
Who is prescribed blood tests?
Let's briefly summarize the factors listed above. The following categories of people need to be tested for vitamin B12:
- elderly people over 60 years of age;
- vegans and vegetarians;
- patients with atrophic gastritis;
- alcohol dependent;
- people with chronic infections;
- patients with neuropsychiatric diseases;
- athletes and people with an active lifestyle.
Additional research is also prescribed if the results of the general analysis are suspicious. If there is a high probability of macrocytic anemia, blood must be taken.
What do the 2 types of megaloblastic anemia have in common and how do they differ?
B vitamins enter the human body with products of animal origin. In the stomach they bind to gastromucoprotein and are absorbed in the small intestine. For normal functioning of the body, the daily dosage of vitamin B12 should be 7 mcg.
The reserve of this vitamin in the liver is no more than 5 mg. The body's need for folic acid is about 100 mcg per day. Vitamin B9 supply up to 10 mg.
Disturbances in the synthesis of DNA molecules lead to the inability of these bone marrow cells to rapidly divide.
These cells include:
- The membranes of the mucous system,
- Digestive tract systems,
- bone marrow cells,
- Skin cells.
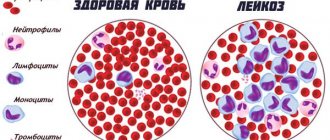
Cells of the hematopoietic system (hematopoietic) are cells that reproduce faster than others. Therefore, indicators (reduced levels of red blood cells and low hemoglobin coefficient) in the hematopoietic system characterize the first manifestations of megaloblastic anemia.
When anemia manifests itself, the following signs of hemolytic anemia are often observed:
- Pathology thrombocytopenia, decrease in the index of platelets in the blood,
- Disease neutropenia, decreased count of neutrophil-type leukocytes,
- Blood pathology agranulocytosis, decreased leukocyte index,
- The disease monocytosis is a decrease in monocyte molecules,
- Decreased reticulocyte synthesis.
The difference and relationship between folate deficiency B9 anemia and vitamin B deficiency B12:
- Vitamin B12 is involved in the synthesis of folic acid molecules. The acid is part of the thymidine molecule, which is a component of the DNA molecule. With the coordinated work of these components, and with their required quantity for the biochemical reaction, the normal formation of blood cells and cells for the normal functioning of the digestive tract occurs,
- The functional responsibilities of vitamin B12 are to help synthesize and break down fatty acids in the body. When there is a deficiency of cyanocobalamin molecules, a disruption in the coordinated reaction occurs, and methylmalonic acid is deposited, which has a detrimental effect on the atoms of neurons. There is also a decrease in the synthesis of myelin, which forms the sheath for nerve cell fibers.
Folic acid does not break down fatty acids and does not participate in the formation of sheaths for nerve fibers.
If there is a deficiency of vitamin B12, the doctor prescribes medications with folic acid, then it activates erythropoiesis, but only until this acid becomes abundant in the body.
An overdose of folic acid occurs:
- Disorder in the nervous system,
- Degenerative changes in the bone spinal cord,
- Combined sclerosis with loss of motor functions,
- Funicular type myelosis.
The importance of cyanocobalamin for the body
Vitamin B12, as mentioned earlier, is responsible for a series of important processes, for example, it not only guarantees the correct formation of nucleic acids - RNA and DNA, prevents the formation of cholesterol plaques in vascular bundles, but also ensures the normal transport of oxygen molecules to all organs and tissues of the body .
Promotes active oxidation of glucose and, as a result, causes elevated blood sugar to return to normal. And also vitamin B12 is necessary for the hematopoietic system. Without it, the correct formation of cellular structures and the stable functioning of red blood cells - blood cells - are impossible. It is worth noting that cyanocobalamin takes part in amino acid metabolism and helps neutralize a number of toxins.
To a greater extent, B12 regulates the activity of the central nervous system (CNS), especially the brain. As soon as the content of cobalamin decreases sharply, its dysfunction immediately occurs - a person begins to have trouble concentrating on details, and it is difficult for him to remember even simple-to-perceive information.
Vitamin B12 enters the body with food, then “settles” in muscle fibers, spleen, liver, intestines and kidneys, forming a kind of depot. If for some reason this substance ceases to be synthesized due to a change in dietary habits, then its supply will be sufficient to lead a full life for 3–7 years (depending on the individual indicators of each individual).
Element B12 is concentrated mainly in food of animal origin, so its consumption is mandatory to maintain health. Dishes with B12 can be safely subjected to heat treatment, as it is resistant to elevated temperatures.
Symptoms of anemia
Symptoms of B12 deficiency anemia and folic acid (as well as its deficiency) are classified according to the following areas in the manifestation of pathology:
- Anemic syndrome in the hematopoietic system,
- Gastroenterological symptoms of disorders in the digestive tract,
- Neurological nature,
- Symptoms of a violation of the structure of the brain.
The classification of anemic direction is manifested in the following symptoms:
- Severe dizziness
- Weakness of the whole body
- State of fainting
- Increased contraction of the heart muscle (sinus tachycardia),
- Dyspnea,
- Painful sensations in the chest,
- Noise in ears,
- Uncertainty in the perception of objects from the visual organs,
- Yellow tint to the skin (the tint gives a high level of bilirubin in the blood).
Gastroenterological symptoms:
- Unreasonable absence of food intake,
- Sudden weight loss
- Severe nausea, which passes into vomiting from the body,
- Diarrhea,
- Constipation,
- The process of inflammation of the oral cavity,
- Burning sensation on the tongue
- The tongue takes on a crimson hue,
- Stomatitis.
Neurological syndrome:
- Biermer anemia, Addison-Beermer disease,
- Mild tingling in fingers and toes
- Constant feeling of chills
- Unsteadiness in movement
- Numbness in the lower extremities,
- Lethargic legs
- The sensitivity of the skin disappears,
- Difficulty in movement.
Deviations in the brain of this type of anemia, as well as disturbances in the functioning of the spinal cord:
- Lack of memory
- Hallucinations,
- State of being lost
- Overexcitement,
- Feeling of constant irritation
- Coma state
- Muscle cramps.
With anemia, lack of vitamin B12, as well as with iron deficiency anemia, signs of severe hypoxia appear in the body:
- Pale skin tone
- Erythropoiesis,
- Peeling on the skin,
- Arrhythmia,
- Angina pectoris
- Swelling,
- Chest pain.
12 deficiency anemia – main symptoms and best treatment methods
› ›
Greetings to all readers of my blog! The topic of today's article is devoted to B12 deficiency anemia, its symptoms and treatment. Here you will find the most important information that will help you quickly restore your health and feel better.
How does deficiency anemia occur?
Vitamin B12 helps form red blood cells. If there is not enough vitamin in the body, anemia develops.
The source of useful substances are products, mainly of animal origin.
In the body, vitamin B12 combines with certain enzymes and enters the blood through the small intestine. Here it combines with a protein that delivers the vitamin to the bone marrow and liver.
If a person eats a balanced diet, then every day his body receives from 30 to 50 mcg of useful substances. The adult liver stores approximately 3-5 mcg of cobalamin (vitamin B12). Therefore, deficiency anemia makes itself felt only a couple of years after the beneficial substance has ceased to be supplied to the body in the required quantity.
Attention! Due to a lack of cobalamin, the process of hematopoiesis is disrupted. As a result, all blood cells are created with some defects in one way or another. If measures are not taken in time, this form of anemia can develop into pancytopenia. When the body experiences a deficiency of all blood elements.
Vitamin B12 deficiency – symptoms
At first, a person suffering from deficiency anemia experiences weakness and gets tired more quickly from usual activities. Over time, symptoms become more severe.
The process of hematopoiesis is disrupted, which manifests itself in the following:
- The skin becomes pale and acquires a yellow tint. This is due to the fact that the destruction of red blood cells reduces the level of hemoglobin and increases the volume of bilirubin.
- The heart begins to beat much faster. This is due to a lack of oxygen. So, the body tries to make up for its deficiency by driving a larger volume of blood through organs and tissues.
- The heart experiences additional stress, so a stabbing pain may occur in the chest area, radiating to the left shoulder and left side of the abdomen.
- During physical activity, dizziness, shortness of breath and even loss of consciousness occur. When a person moves actively, the muscles of his body need more energy, and in order for it to be produced, more oxygen is needed. Therefore, the heart increases its contraction rate. In people with vitamin B12 deficiency, the heart already works at increased speed, and additional physical activity only worsens their well-being.
- Dizziness and loss of consciousness are common. This indicates that the brain is not receiving enough oxygen.
- Vision deteriorates, “midges” appear before the eyes. The organs of vision experience oxygen starvation due to insufficient blood flow. This disrupts metabolism, so a person begins to see worse.
- Ultrasound shows an enlarged spleen because large red blood cells clog its capillaries.
With a deficiency of vitamin B12, the digestive system is one of the first to suffer, as the mucous membranes stop producing enzymes to break down food in sufficient quantities. The body does not have enough nutrients, so the following problems arise:
- Bowel disorder (diarrhea or diarrhea)
- Heartburn
- Poor appetite
- Weight loss
- Bloating
- Gradually, the tongue becomes bright crimson and smooth
- The mucous membrane of the tongue atrophies, therefore taste sensations are distorted
- Increased risk of infections in the mouth
- Pain and burning sensation appear in the oral cavity
- After eating, you may experience abdominal pain. Especially if the person has eaten spicy foods, rough or poorly processed foods
Myelin sheaths, which are part of nerve fibers, are formed with the help of vitamin B12. That is why it is so important for the full functioning of the nervous system. As a result of a lack of useful substances, the brain and spinal cord cope with their functions worse. This manifests itself in the following symptoms:
- Reduced sensitivity to cold, heat and even pain in different parts of the body
- Tingling in fingers and wrists
- Impaired coordination of movements
- Muscle weakness. If the disease progresses, the person will not be able to control his body
- The patient loses control over urination and bowel movements
- Insomnia
- Bad memory
- Depression
- Psycho-emotional disorders
- Hallucinations
- Convulsions
Why does cobalamin deficiency occur?
The causes of deficiency anemia are quite varied, including:
- Diet without enough meat and dairy products. For example, when a person follows a strict diet or practices vegetarianism. Vegetarian mothers are more likely to experience anemia in their infants.
- Poor absorption of cobalamin
- Insufficient amount of protein (Castle factor), which is necessary for the absorption of vitamin B12 in the stomach. One of the reasons for this problem is antibodies that destroy cells in the stomach that produce this type of protein. Also, protein deficiency can be caused by inflammatory processes in the stomach, taking certain medications, alcohol, gastritis, gastric surgery and congenital disorders.
- Damage to the intestine caused by surgical intervention, aggressive action of microorganisms, disruption of microflora and malignant neoplasms.
- Worms and bacteria in the gastrointestinal tract, for which B12 serves as food.
- Inadequate functioning of the liver, kidneys and other organs that are involved in the absorption of vitamin B12.
- In some cases, the body needs an increased amount of vitamin B12. For example, in infancy, with increased production of thyroid hormones and with an insufficient number of red blood cells (erythrocytes).
Elderly people and those with stomach problems are more likely than others to experience deficiency anemia.
Treatment options
In order to replenish the supply of cobalamin in the body, it is necessary to eliminate the cause of its deficiency.
- The patient may need to remove worms from the body, or remove the tumor or change the diet.
- Additional intake of vitamin B12 in the form of intramuscular injections from 200 to 500 mcg daily. As soon as a positive and stable result is achieved, the dosage is reduced to 100-200 mcg. Injections are administered once every 30 days, for several months in a row.
- In an anemic coma, when the patient loses an adequate reaction due to oxygen deficiency, a transfusion of donor red blood cells obtained from blood is prescribed. Also, this method is used when the hemoglobin level drops below 70 g/l. Both of these conditions are dangerously lethal!
How to prevent deficiency anemia?
Prevention of vitamin B12 deficiency consists of the following rules:
- Be sure to include beef liver, low-fat milk powder, hard cheese, dairy products, beef, pork, chicken, seafood, sardines, homemade soft cheese, egg yolks, sprouted wheat, spinach and seaweed in your diet.
- Take natural supplements regularly. For example, the Ultivit vitamin complex contains not only vitamin B12, but also other vital substances that are necessary for the body to function properly and maintain good health. It is taken for prevention and in addition to the treatment of cobalamin deficiency.
BoostIron is widely used to prevent and eliminate anemia, as it contains non-toxic iron, vitamin B12, vitamin C and folic acid.
Both products are certified in Europe, the USA and Russia, but the most important thing is that they are approved by famous doctors and included in health programs for children, athletes and pregnant women.
By coupon number - 1117 , all readers of my blog receive a 5% discount and favorable delivery conditions!
- To avoid vitamin B12 deficiency, regularly carry out preventive cleaning of parasites and worms. It is better to do this with the help of natural plant-based products. Black Walnut works very effectively and at the same time gently. It destroys parasites and helminths in the gastrointestinal tract and removes them from the body. But this is not the only advantage of Black Walnut; it saturates the body with useful substances, cleanses the skin and improves digestion. Follow the link and you will learn more about it.
- If you have had part of your intestines or stomach removed, you need to not only monitor your diet, but also take supplements with vitamin B12, such as those I wrote above.
Diagnostic methods
- First of all, the doctor examines the patient and collects anamnesis. In simple words, it asks questions about lifestyle, symptoms, concomitant diseases, etc. Also, pulse rate and blood pressure are measured.
- Then, a general blood test, a urine test (to identify other diseases), an analysis for the level of cobalamin in the blood and biochemical parameters are prescribed.
- In order to determine how much vitamin B12 is contained in the bone marrow, a bone puncture may be prescribed.
- To determine the heart rhythm, an ECG (electrocardiography) is performed.
Why is vitamin B12 deficiency dangerous?
B12 deficiency anemia can lead to the following complications:
- Numbness of the arms and legs, muscle weakness, urinary and fecal incontinence, loss of sensation in various parts of the body and impaired coordination of movements. This occurs due to damage to the spinal cord and peripheral nerves.
- Coma. Occurs as a result of oxygen starvation of the brain.
- Violation of the functions of internal organs.
If deficiency anemia is not treated promptly, its consequences may be irreversible!
Today, I told you about B12 deficiency anemia, its symptoms and treatment methods. Therefore, I am confident that you will take all necessary measures to avoid serious health problems.
I sincerely wish you good health and good health! Take care of yourself.
B 12 deficiency anemia - main symptoms and best treatment methods Link to main publication
Source: https://anemiya.su/b-12-defitsitnaya-anemiya-osnovnye-simptomy-i-luchshie-metody-lecheniya
Forms of development
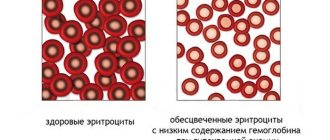
The pathogenesis of anemia occurs when there is insufficient loss of B vitamin molecules into the body, namely B12 and B9, which affects the level of hemoglobin molecules, which are located in red blood cells and are responsible for the delivery of oxygen atoms to all cells of the human body.
Anemia is divided into forms according to the index of hemoglobin molecules in the blood plasma.
The lower the hemoglobin index, the more severe the degree of deficiency pathology:
- Light stage of development and course of hemoglobin index from 90.0 to 110.0 grams per liter of biological fluid,
- Moderate hemoglobin index from 70.0 to 90.0 grams per liter of blood plasma,
- In the severe stage of this pathology, the red pigment coefficient does not exceed 70.0 and decreases even below this indicator.
Standard indicators for the amount of hemoglobin in the blood of men are 130.0 160.0 g/l.
For women, the standard is 120.0 135.0 g/l.
B12 deficiency anemia in children
The main types of etiology of anemia with a lack of this vitamin in childhood are:
- Changes in the baby's microflora,
- There is not enough of this vitamin in the child’s body,
- The presence of worms in the body,
- Castle factor during the period of intensive child growth.
Clinical indicators and manifestations of this type of pathology are similar to the symptoms of an adult, but there are characteristic symptoms in a child’s body:
- Severe dental caries from a young age,
- Persistent stomatitis that begins in infancy,
- Changes in the eyeball
- Changes in the nail plate: the plate is weak, brittle,
- Impaired attention and intelligence, decreased performance at school.
In transcripts of clinical laboratory results, the following values are:
- Low hemoglobin index,
- Reduced number of red blood cell molecules,
- The color index is increased by more than 1.5,
- In the molecules of erythrocytes, Cabot rings, as well as Jolly bodies, are present in such quantities that they are determined by analysis,
- Reticulocytes are increased
- Increased lymphocyte count,
- Platelets, as well as leukocytes in small quantities,
- Biochemistry revealed megaloblasts as part of a bone marrow puncture.
To help laboratory indicators, to establish a diagnosis of B12 deficiency anemia, an instrumental method for diagnosing the child’s body is used:
- Ultrasound of liver cells,
- Ultrasound of spleen cells,
- Gastroendoscopy of the alimentary tract and intestines,
- Irrigoscopy of the small part of the intestine,
- Colonoscopy checks the condition of the colon.
Treatment of anemia in a child with B12 deficiency involves saturating the body's cells with these vitamins. Medication vitamin course 15 calendar days. A high-calorie diet is also prescribed, which contains foods with vitamin B12 and folic acid.
To replenish vitamin molecules in the body, the drug Cyanocobalamin is prescribed. The initial dosage of this drug is from 30.0 mcg to 50.0 mcg, when taken daily. This drug is administered orally by injection.
The dosage is calculated individually by the attending doctor. The medication course is carried out in children under the strict supervision of a specialized specialist.
After completing the course of treatment for preventive purposes and as maintenance treatment, 100.0 250.0 mcg 2 times a month.
Standard indicators of vitamin cyanocobalamin in the child’s body:
age of the child norm per day of vitamin cyanocobalamin
| from birth to 6 months of age | 0.40 mcg |
| from 6 calendar months to one year | 0.50 mcg |
| at one year of age and up to the 3rd birthday | 1.0 mcg |
| from 3 calendar years to 6 years | 1.50 mcg |
| from the age of six to the 10th birthday | 2.0 mcg |
Etiology
Vitamin B12 benefits the body when it is absorbed in the intestines. For this absorption reaction to occur, an enzyme is needed, which is produced by the internal parts of the stomach - Castle's enzyme.
Without the formation of an enzyme, vitamin B12 molecules are excreted outside the body without entering it for biochemical processes, through feces.
With B12 deficiency anemia, the Castle enzyme is not synthesized in the stomach, so the vitamin that gets into food is also not absorbed through the intestines.
Liver cells contain a reserve of vitamin B12 molecules, which, if used wisely, can be sufficient for 5 calendar years. As a result, anemia occurs some time after the stomach has stopped producing this factor.
Castle factor deficiency is the main cause of the pathology of B12 deficiency anemia.
Symptoms of anemia
Symptoms of vitamin B12 deficiency are divided into three types: anemic group of symptoms, gastroenterological and neurological.
The anemic group includes weakness, fatigue, fainting, dizziness, chest pain, and high blood pressure. The gastroenterological group includes sudden weight loss, vomiting, diarrhea, lack of appetite, constipation. At an advanced stage of the disease, a neurological syndrome appears. It is accompanied by symptoms such as numbness of the limbs, impaired gross and fine motor skills, stiffness in movements, convulsions, and increased irritability.
Causes
Lack of cyanocobalamin is caused by the following factors:
- Low content of foods with vitamin B12 in food (the main reason) . Cyanocobalamin is found in foods of animal origin. Vegetarianism is the main risk factor for B12 deficiency in food.
- Castle factor function is impaired . With atrophy of the cells of the mucous membranes, the functionality of the internal factor does not manifest itself, or it decreases. This cause of atrophy can be genetic, congenital, with gastritis of the stomach, when the stomach is exposed to toxic elements (intoxication of the body), as well as the effect on the antibody factor,
- Absence or partial loss of receptors that are necessary for the factor . This pathology develops with Crohn's disease, with neoplasms in the small intestine (cancer), with tuberculosis, with intestinal infantilism, as well as with enteritis in the chronic stage of the pathology,
- Absorption of B12 molecules by worms and pathogenic microorganisms . This pathology must be treated with therapy against competitors that absorb cyanocobalamin,
- With pathology of the pancreas . With this pathology, there is a deviation in the breakdown of the protein protein, which is the link between the factor and vitamin B12,
- A genetic hereditary congenital anomaly is a reduced rate of transcobalamin synthesis in the body, which leads to a disruption in the transport of cyanocobalamin molecules into bone marrow cells.
For folate deficiency anemia, the etiology with food is not suitable, because vitamin B9 is present in every food of plant and animal origin. This B vitamin does not require the help of a factor and is absorbed independently.
Folio deficiency problems begin when the following causes appear in the body:
- Poor diet
- Low food consumption
- Starvation,
- Anorexia,
- The patient is elderly, at this age it is difficult to absorb vitamins from food,
- Drinking alcoholic beverages. With alcohol addiction, a person cannot eat properly,
- Pathology in the intestines, which does not allow vitamins to be absorbed by the body,
- Crohn's disease
- Blood hemogram,
- Pathology of celiac disease,
- Malignant neoplasms in the intestines,
- Increased need for vitamin B12 and folic acid in a woman during the period of intrauterine formation of the baby. In pregnant women, dietary intake of these products should be increased to avoid fetal hypoxia,
- Increased consumption of B9 in the pathology of psoriasis,
- When taking anticonvulsant medications, a deficiency of vitamin B9 and B12 occurs.
Vitamin deficiency occurs when taking medications
Vitamin B12 deficiency: symptoms, diagnosis, treatment
- Reducing dietary intake
- Decreased breakdown of vitamin B12 from food in the stomach
- Malabsorption from the gastrointestinal tract
Patients at high risk of vitamin B12 deficiency include:
- Vegans
- Persons with a history of surgery in the stomach or intestines
- Persons with a history of atrophic gastritis
- Pernicious anemia, a condition in which autoimmune destruction of the parietal cells that produce intrinsic factor leads to decreased absorption of vitamin B12 from the gastrointestinal tract
- Malabsorption from the gastrointestinal tract.
Drugs that reduce the breakdown of vitamin B12 from foods (acid-blocking drugs and proton pump inhibitors) or reduce the absorption of vitamin B12 (metformin) can also cause vitamin B12 deficiency.
Any malabsorption syndrome may also put the patient at risk of developing vitamin B12 deficiency, for example:
- Crohn's disease
- Celiac disease
- Bacterial overgrowth syndrome.
The relationship with patients infected with Helicobacter pylori is unknown, but a possible connection with atrophic gastritis, which reduces the ability to break down vitamin B12 from food.
Pathophysiology
Consume food sources of vitamin B12 (meat, poultry, dairy products), which is extracted from food under the action of gastric juice. Free vitamin B12 then binds to intrinsic factor (IF), which is produced by the parietal cells of the fundus of the stomach. The vitamin B12-VF complex then travels to the small intestine where endocytosis occurs in the terminal ileum, during which it binds to transcobalamin. The transcobalamin-vitamin B12 complex (holotranscobalamin) is then released into the serum for use by cells. Any impact on this process may put the patient at risk of vitamin B12 deficiency.
Vitamin B12 is an essential cofactor for DNA synthesis and is closely related to folate metabolism. In particular, vitamin B12 acts as an important cofactor in 2 specific biomechanical processes in which methylmalonic acid and homocysteine participate as precursors. Vitamin B12 deficiency impairs the conversion of methylmalonic acid to succinyl-coenzyme A. Vitamin B12 or folate deficiency impairs the conversion of homocysteine to methionine. Methionine is required for the production of S-adenosylmethionine, which plays an important role in neuronal function. Vitamin B12 and folate are considered integral to normal hematopoiesis and bone marrow function.
Thus, long-term and severe vitamin B12 deficiency can cause neurological and hematological disorders. A relationship has also been noted between psychiatric diseases (dementia, depression, cognitive impairment) and vitamin B12 deficiency.
Diagnostics
Traditionally, the diagnosis of vitamin B12 deficiency is based on low serum levels of vitamin B12 (usually <200 pg/mL) and clinical symptoms that indicate vitamin B12 deficiency. Unfortunately, the neurological diseases that are associated with vitamin B12 deficiency may be irreversible, and early detection can be critical in preventing permanent neurological damage. Additionally, there is no consensus regarding the normal serum level of vitamin B12 for optimal neurological and hematological function.
The use of tissue deficiency markers such as homocysteine, methylmalonic acid (MMA) and holotranscobalamin improves the early diagnosis of vitamin B12 deficiency. The optimal use of serum vitamin B12 levels and tissue markers has not been determined, but the general guidelines presented will help the clinician determine whether a patient is actually vitamin B12 deficient.
At-risk groups
Your doctor should consider some risk factors when ordering testing for vitamin B12 deficiency. Older age is associated with increased risk. Also at risk for deficiency are patients who use medications for a long time (especially metformin, proton pump inhibitors and anticonvulsants). In addition, patients with chronic gastrointestinal diseases that may cause malabsorption or insufficient absorption, including Crohn's disease and celiac disease, as well as patients with upper gastrointestinal surgery, including gastrectomy, gastric bypass, should be screened for vitamin B12 deficiency. or ileal resection.
Symptoms and signs
Patients with unexplained neurological disease (especially decreased vibration sensitivity, gait disturbance and peripheral neuropathy) should be tested for vitamin B12 deficiency. Neuropsychiatric complaints such as depression and dementia may also indicate to the doctor an underlying vitamin B12 deficiency. Late signs of vitamin B12 deficiency include angular stomatitis, glossitis of the tongue and signs of severe anemia and thrombocytopenia.
Primary diagnostic tests
Serum vitamin B12 remains a reasonable initial diagnostic test for vitamin B12 deficiency due to its widespread availability and awareness. However, caution should be exercised when interpreting the results, as there are no generally accepted cutoff values.
In general, serum vitamin B12 levels can be broken down into 3 values:
- Probable vitamin B12 deficiency: <148 pmol/L (<200 pg/ml)
- Possible vitamin B12 deficiency: 148–258 pmol/L (201–350 pg/ml)
- Unlikely vitamin B12 deficiency: >258 pmol/L (>350 pg/ml)
A CBC with a peripheral blood smear is useful to determine the presence of macrocytosis and significant anemia, leukopenia, or thrombocytopenia. This result indicates a more severe and long-lasting vitamin B12 deficiency. However, normal values for mean red blood cell volume, hemoglobin, and hematocrit do not help exclude tissue vitamin B12 deficiency, since many patients with vitamin B12 deficiency may have normal hematological parameters.
A peripheral blood smear may reveal the classic hypersegmented polymorphonuclear cells and megalocytes found in severe vitamin B12 deficiency with associated macrocytic anemia, but is insensitive in detecting early vitamin B12 deficiency.
Assessment of serum folate levels has previously been recommended because low serum folate levels may falsely underestimate serum vitamin B12 levels. However, during times of folic acid fortification, concomitant folate deficiency is rarely observed. In countries around the world where malnutrition is common, testing for concomitant folate deficiency and its treatment can help identify actual vitamin B12 deficiency.
Clinical assessment of deficiency severity
The severity of the deficiency from a clinical point of view can be classified as follows:
- Mild to moderate neurological manifestations: dysesthesia/paresthesia, polyneuropathy and depression
- Mild to moderate hematologic manifestations: Typically asymptomatic with normal hematocrit and high normal or slightly elevated mean red cell volume.
- Severe neurological manifestations: subacute combined spinal cord degeneration, dementia or cognitive impairment. Subacute combined spinal cord degeneration is a progressive neurological degeneration of the posterior and lateral columns of the spinal cord. Patients experience ataxia, decreased vibration sensitivity, muscle weakness and hyporeflexia.
- Severe hematological manifestations: pancytopenia and severe symptomatic anemia.
Confirmatory diagnostic studies
Serum vitamin B12 <148 pmol/L (<200 pg/mL): confirmatory treatment is usually not required and empirical treatment should be initiated. The clinical and serological response from follow-up confirms vitamin B12 deficiency.
Serum vitamin B12 148–258 pmol/L (201–350 pg/mL): MMC can be extremely sensitive to vitamin B12 deficiency, but falsely high levels may be observed in kidney disease. In addition, the level of MMC, which does not correspond to the norm, has not been established. Patients with serum vitamin B12 levels in this range, along with elevated SUA levels, can be considered to have probable vitamin B12 deficiency. The diagnosis is confirmed if vitamin levels return to normal and serum vitamin B12 levels increase with appropriate treatment with vitamin B12.
Homocysteine: Levels may be elevated in folate deficiency, hypothyroidism, and vitamin B12 deficiency. Patients with elevated homocysteine levels associated with vitamin B12 deficiency (when folate deficiency and hypothyroidism have been excluded) should be normalized with empirical treatment with vitamin B12.
Holotranscobalamin (hTC): This marker is being studied as a more specific marker of vitamin B12 absorption capacity. hTC is a transcobalamin bound to vitamin B12, which can serve as a measure of actual functional levels of vitamin B12 in serum. hTC may be the first marker detected for vitamin B12 deficiency. HTC levels <35 pg/L may be consistent with vitamin B12 deficiency and may be considered, but this test is not widely available.
Antiparietal cell antibodies (APC): Once vitamin B12 deficiency is confirmed, APC can be determined if the cause of the deficiency is pernicious anemia (PA). This analysis is characterized by high sensitivity (85%), but it is nonspecific, since the level of APC can be increased in atrophic gastritis.
Fasting serum gastrin levels: Gastrin levels are elevated in gastric achlorhydria and may indicate PA.
Determining the root cause of vitamin B12 deficiency
Once vitamin B12 deficiency is discovered, the etiology should be considered. Although treatment remains the same, vitamin B12 deficiency may lead the careful clinician to look for malabsorption as the underlying disorder, such as in celiac disease or Crohn's disease.
Diagnosis of pernicious anemia:
- Antibodies to intrinsic factor have only 50% sensitivity, but are highly specific for pernicious anemia.
- Antibodies to parietal cells are very sensitive (85%), but are not specific, as they may increase in pernicious anemia.
- Serum gastrin levels (measured in the fasting state) increase sharply with gastric achlorhydria and may indicate pernicious anemia.
The Schilling test is a classic test for determining vitamin B12 absorption, but it is not widely used due to the difficulty of performing and obtaining radioisotopes of vitamin B12.
Differential diagnosis
| Disease | Differential signs/symptoms | Differential examinations |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Treatment
Patients with severe hematological or neurological symptoms of vitamin B12 deficiency require immediate intensive treatment with cyanocobalamin or hydroxocobalamin for more than 1 month, after which maintenance doses of the drug are prescribed. Patients with mild to moderate symptoms of vitamin B12 deficiency should begin and continue treatment with maintenance doses of cyanocobalamin. Asymptomatic patients at high risk of vitamin B12 deficiency (eg, vegans and vegetarians, elderly patients, those with chronic gastrointestinal diseases) also require treatment because the hematologic and neurologic complications of vitamin B12 deficiency may be irreversible. If the cause of vitamin B12 deficiency has not yet been determined, treatment should still be started while further research is carried out.
Vitamin B12 Therapy Options
May be administered parenterally (intramuscular [IM] or subcutaneous [SC]), orally, sublingually, or intranasally. Today, the most reliable and most often used method for treating vitamin B12 deficiency is the parenteral method of administration (i.m. or s.c.). Patients with severe anemia and/or neurological disease (subacute combined spinal cord degeneration, dementia or cognitive impairment) should be given IM injections daily or every other day for the first 2 to 4 weeks. Typically, subsequent maintenance doses are given monthly.
Studies since 1960 have shown that oral vitamin B12 in the form of cyanocobalamin in high doses can be absorbed even in patients with pernicious anemia or massive resection of the terminal ileum. A small percentage of oral vitamin B12 is absorbed by passive diffusion, regardless of the presence of intrinsic factor or an intact terminal ileum. There is renewed interest in oral supplementation for vitamin B12 deficiency, giving clinicians more treatment options.
In patients with vitamin B12 deficiency (in a meta-analysis), oral cyanocobalamin was as effective, if not more effective. Although absorption occurs at dosages <1000 mcg/day, the intensity of absorption is likely to fluctuate and the clinical and laboratory response is less than maximal. Absorption increases when administered on an empty stomach.
Bariatric surgery patients may not receive enough multivitamins to maintain serum vitamin B12 levels and should be given cyanocobalamin, either orally, parenterally, or intranasally.
Studies comparing sublingual cyanocobalamin with oral cyanocobalamin and intranasal cyanocobalamin have shown efficacy. However, sublingual or intranasal cyanocobalamin should not generally be used to treat vitamin B12 deficiency due to limited evidence and knowledge regarding its optimal dosage.
Presence of symptoms
Severe symptoms
- Patients with severe hematological (pancytopenia and severe symptomatic anemia) or neurological (subacute combined spinal cord degeneration, dementia or dementia) symptoms of vitamin B12 deficiency require urgent treatment.
- Patients with pernicious anemia and pancytopenia should be hospitalized and consulted with a hematologist, and red blood cell transfusions may rarely be required. If signs of congestive heart failure occur, red blood cells should be transfused along with a low dose of diuretics. In an intensive treatment regimen, cyanocobalamin is administered parenterally at a dose of 1000 mcg daily for 1–2 weeks, and then 1000 mcg parenterally once a week until the 1st month until severe reticulocytosis occurs in the bone marrow. The addition of folic acid helps eliminate hematological disorders.
- At the beginning of an intensive parenteral treatment regimen, patients with severe neurological symptoms may require consultation and evaluation by a neurologist and psychogeriatrician. In some cases, despite normalization of serum vitamin B12, neurological symptoms may be irreversible.
- Maintenance therapy continues with oral cyanocobalamin (once daily) or parenteral cyanocobalamin (once monthly).
Mild to moderate symptoms
- Intensive and supportive therapy for patients with mild to moderate symptoms of vitamin B12 deficiency (hematological: mild anemia; neurological: dysesthesia/paresthesia, polyneuropathy, depression) is carried out with oral cyanocobalamin (once daily) or parenteral cyanocobalamin (once monthly).
- In patients treated with oral cyanocobalamin, response should occur within 2 months. If serum vitamin B12 levels do not rise significantly after 2 months of daily oral cyanocobalamin, the doctor changes therapy to intramuscular vitamin B12 or looks for other causes.
Asymptomatic or borderline deficiency
Patients at high risk for vitamin B12 deficiency should be monitored and, even in the absence of symptoms, treated with cyanocobalamin (oral or parenteral). This is because the hematological and neurological complications of vitamin B12 deficiency may be irreversible. In the UK, patients with borderline serum cobalamin levels (subclinical values) are advised to receive an empirical trial of low-dose cyanocobalamin for 1 month on two occasions.
Treatment for older patients includes dietary advice about the importance of eating animal products such as meat, fish, eggs and milk, as well as multivitamin supplements. Those on restrictive diets, such as vegans and vegetarians, should be aware that they may require monitoring and dietary supplements for the rest of their lives. Infants of vegan mothers require supplements from birth.
Parenteral cyanocobalamin should be prescribed to patients with chronic gastrointestinal diseases that may cause malabsorption or inadequate absorption, such as pernicious anemia, gastric surgery, gastric bypass, Crohn's disease, terminal iliectomy, and celiac disease.
Monitoring and response to treatment
In patients with severe anemia caused by vitamin B12 deficiency, a reticulocyte surge in the bone marrow occurs in response to treatment, which can be measured in 1 to 2 weeks. Other signs of deficiency, including methylmalonic acid, homocysteine, and MCV, should normalize after 8 weeks of adequate treatment. Serum vitamin B12 (serum cobalamin) should be normalized before initiating maintenance therapy.
Diagnostics
When making this diagnosis of B12 deficiency anemia, the doctor first of all during diagnosis collects an anamnesis when and under what circumstances the pronounced symptoms of anemia appeared, with its weakness and manifestations of pathology in the digestive process.
It is also necessary to find out whether the patient has diseases that occur in a chronic stage, as well as to provide information about possible genetic hereditary congenital diseases.
After the medical history, the patient’s skin is examined and pronounced symptoms on the skin are determined.
The doctor also measures the blood pressure index (in anemia, the pressure is low), as well as the heart pulse (often the pulse is rapid).
After this examination, based on external signs, laboratory diagnostics (blood tests) are prescribed, as well as a list of instrumental studies:
- General blood analysis,
- Biochemical analysis of blood composition,
- Urine for general analysis,
- Bone marrow puncture,
- Electrocardiography (ECG),
- Ultrasound of the liver and spleen,
- Ultrasound of the intestines,
- Ultrasound of the stomach.
When deciphering the general analysis, the whole picture of the blood is visible, the indicators of each element in its composition. According to this analysis, in vitamin B12 deficiency anemia, a decrease in red blood cell molecules is seen, as well as a decreased synthesis of reticulocytes.
The level of red pigment (hemoglobin) is reduced, platelets are also reduced, which provokes hypoxia. Color increases with anemia and reaches more than 1.50 (with the norm being 0.860 - 1.050).
During the analysis, the presence of proteins in urine is observed, and possible detection of concomitant pathologies.
Biochemistry is the most valuable analysis for identifying deviations in the structure and composition of the blood.
Biochemistry reveals the following indicators for B12 deficiency anemia:
- The cholesterol index is often elevated in anemia,
- The presence of creatinine
- Glucose in the blood
- Uric acid,
- Electrolyte indicators of calcium, potassium and sodium molecules,
- Lactate dehydrogenase is an enzyme found in liver cells that promotes the absorption of iron by cells. Indicator of biological reactions for the synthesis of red blood cells and hemoglobin,
- B vitamins are reduced. The B12 index is low.
A blood hemogram shows the hematocrit number, the percentage of all types of leukocytes is determined by the leukocyte formula.
A myelogram, or bone marrow puncture indicators, determines the level of production of red blood cell molecules, as well as megaloblasts in the blood, which confirms the megaloblastic nature of hematopoiesis in the human body.
The instrumental technique determines deviations from standard indicators in the structure of internal organs, and also identifies violations in their functionality.
What should be the normal level of B12 in the blood?
When assessing the test results, the average level of vitamin B12 in the blood is taken into account. The norm depends on age and is given in two parameters - ng/l, pmol/l. The indicators are as follows:
- From zero to one year - 216-891 pmol/l or 293-1207 ng/l .
- From two to three years - 195-898 pmol/l or 265-1215 ng/l .
- From four to six years - 181-795 pmol/l or 245-1077 ng/l .
- From seven to nine years - 200-863 pmol/l or 271-1173 ng/l .
- From ten to twelve years - 135-803 pmol/l or 183-1080 ng/l .
- From thirteen to eighteen years - 158-638 pmol/l or 214-864 ng/l .
- From 18 years and over - 148-738 pmol/l or 200-1000 ng/l .
If we consider vitamin B12 in general, the norm in the blood for women and men differs slightly.
To convert from one parameter to another, you should use the following formula: ng/l = (pmol/l)/0.738. It is important to note that different laboratories may use individual reagents, therefore the standards are adjusted in one direction or another.
Most often, decryption is done as follows:
- A reading above 300 ng/l means a vitamin deficiency is excluded.
- 200-300 ng/l - it is worth checking the level of methylmalonic acid. If it increases, B12 treatment is prescribed.
- Up to 200 ng/l - the diagnosis of cobalamin deficiency is confirmed.
An analysis for the level of B12 in the blood is often carried out in conjunction with other studies:
- General blood analysis.
- Antibodies to parietal cells and intrinsic factor.
- Reticulocyte analysis.
- Ferritin.
- Leukocyte formula.
- Homocysteine.
Therapy for B12 deficiency anemia
Therapy for B12 deficiency anemia begins with treatment of the root cause of this deficiency: therapeutic therapy to destroy helminths, normal and balanced nutrition, as well as surgical methods for treating malignant neoplasms.
For the complex treatment of anemia, the drug B12 is administered into the body at a dosage of 200.0 mcg 250.0 mcg per day. The drug is injected into muscle tissue, or injected under the skin of the human body.
If anemia has affected the centers of the nervous system, then the drug therapy regimen is as follows: for the first 3 calendar days, a vitamin dosage of 1000.0 mcg per day, and subsequent treatment according to the prescribed regimen. The treatment regimen, as well as the dosage of B12, is prescribed by the attending doctor and depends on the degree of deficiency in the body of vitamin B12, which caused anemia.
After stabilization of this vitamin in the body, to maintain it at a normal level, B12 preparation is used in treatment at 100.0 mcg 200.0 mcg 1 time per calendar month.
Clinical recommendations for the rapid replenishment of red blood cells in the blood include intravenous administration of red blood cells, which can restore the destroyed balance in the composition of the blood plasma of the human body.
Treatment
Treatment of folic acid deficiency is predominantly limited to the administration of tablet forms of vitamin B9 at a dose of 5-15 mg/day. However, if the diagnosis of folate deficiency anemia still remains in question, then it is advisable to begin treatment with intramuscular administration of cyanocobalamin. However, the opposite is not possible, because with B12-deficiency anemia, the use of folic acid will further aggravate the situation.
As for the treatment of B12 deficiency anemia, it is based on three principles:
- Fully saturate the body with cyanocobalamin, so that it will be enough to perform functional duties and be put aside in reserve;
- Constantly replenish supplies using maintenance doses;
- If possible, try to prevent the development of an anemic state.
It goes without saying that the main thing in the treatment of B12 deficiency will be the administration of cyanocobalamin, taking into account changes in the blood and the severity of neurological symptoms, if any.
Thus:
- Treatment usually begins with intramuscular administration of cyanocobalamin at a dose of 500 mcg every day and oxycobalamin - 1000 mcg every other day;
- If there are severe symptoms of damage to the nervous system (funicular myelosis), then the dose of B12 is increased to 1000 mcg (every day), and, in addition, 500 mcg of adenosylcobalamin tablets are added, which takes part in the metabolism, but does not affect hematopoiesis;
- The appearance of hypochromia of red blood cells in a blood test during treatment or in the case of mixed forms of the disease (B12- + iron deficiency anemia) is the basis for prescribing iron supplements;
- Transfusion of red blood cells is resorted to in special cases: if signs of oxygen starvation of the brain and symptoms of anemic encephalopathy are clearly visible, there is progressive heart failure and if the development of an anemic coma is suspected - a very life-threatening condition for the patient;
- At the same time, a therapeutic effect is prescribed on factors that may have caused vitamin B12 deficiency, for this purpose the following is carried out: deworming (drugs and doses depend on the type of helminths), treatment of diseases of the gastrointestinal tract, surgery for stomach cancer, normalization of intestinal flora, A diet is being developed that provides a sufficient supply of vitamin B12 to the body.
Literally a few days after the start of therapy, a control count of reticulocytes is performed - a reticulocyte crisis will be evidence that the treatment tactics have been chosen correctly.
After the blood condition is considered normal, the patient is transferred to maintenance therapy: first, every week, and then every month, the patient is administered 500 mcg of B12, and, in addition, every six months, a 2-3 week course of vitamin therapy is prescribed (maintenance treatment with vitamin B12 ).
Foods rich in vitamin B12 (only for the prevention of anemia associated with a lack of cyanocobalamin in food):
Complicated form of B12 deficiency anemia
If emergency treatment measures are not taken, the consequences of this type of anemia can be quite serious and pose a threat to the patient’s life:
- Comatose state in which the patient does not respond to external stimuli. Coma can occur from cerebral hypoxia during anemia and can cause death,
- Severe degree of anemia , which significantly worsens the condition of the body and triggers irreversible consequences in it. This degree occurs when the hemoglobin index is lower than 70.0 g/l,
- Funicular myelosis is a lesion of the cells of the spinal cord, as well as the nerve endings of the peripheral parts of the body. Damage to the connecting nerve fibers of the spinal cord with the centers of the brain, as well as with all internal organs and systems of the body. With these disorders, the sensitivity of the limbs decreases, unsteadiness in movements appears, and as myelosis progresses, sensitivity disappears completely and the person is not able to move independently,
- Destruction of cells of internal organs , which subsequently leads to non-functionality of this organ (the heart, liver and spleen cells, digestive tract, kidney cells, respiratory system are affected).
If the treatment process begins too late, then complications in the nervous system cannot be restored. These destructions are irreversible.
Prevention
Prevention is mainly aimed at improving B12 intake through foods:
- Consumption of animal products containing large amounts of B12,
- Timely treatment of pathologies that can cause B12 deficiency and provoke anemia,
- After surgery on the digestive tract, take medications to maintain the level of this vitamin.
Foods rich in vitamin B12
Indications for use, features of the analysis
Testing your cobalamin level is recommended in the following cases:
- atrophic gastritis;
- chronic inflammatory diseases;
- anatomical defects of the small intestine;
- for diagnosing anemia;
- when checking for congenital forms of B12 deficiency.
The greatest interest is in determining the level of vitamin B12 in the blood (cyanocobalamin norm). The algorithm is as follows:
- At the first stage, a blood test is performed in the laboratory to determine the vitamin content.
- Next, the patient receives cyanocobalamin, and after some time the test is performed again.
- A slight increase in B12 content indicates problems with digestibility, which is often caused by gastrointestinal diseases. If the study gives such results, then a wider examination of the patient is prescribed to identify the exact causes of malabsorption.
Diet for this form of anemia
A balanced diet is especially necessary during the period of intrauterine development of a child, since the formation of the baby, as well as the occurrence of intrauterine pathologies that are revealed after birth, depend on the intake of vitamins in the body of a pregnant woman.
During pregnancy, the need for vitamin B12 increases by 50.0%.
products; amount of B12 in mcg
| · calf liver | · 60,0 |
| liver of a young piglet | · 30,0 |
| chicken liver | · 16,0 |
| · mackerel fish | · 12,0 |
| · rabbit meat | · 4,30 |
| · veal | · 2,60 |
| · perch fish | · 2,40 |
| · pork | · 2,0 |
| · eggs | · 0,40 |
| · fat sour cream |
For B12 deficiency anemia, diet table No. 11 is used. This diet should increase the content of protein and vitamin B12 in the body. The food preparation method is standard. You need to eat 5 times a day.
Energy value of diet No. 11:
- Proteins 110.0 grams 130.0 grams (60.0% animal origin, 40.0% plant origin),
- Fats 100.0 grams 120.0 grams (80.0% animal and only 20.0% vegetable),
- Carbohydrates 400.0 grams 450.0 grams,
- Salt no more than 15.0 grams,
- Purified water 1.5 liters.
products useful for B12 deficiency anemia; prohibited products
| · veal, pork, chicken liver | · milk |
| · salo | · baking |
| · butter | · confectionery sweet products |
| · mackerel fish | · tea |
| · meat: veal, rabbit, pork | caffeinated drinks |
| · eggs | · Coca Cola |
| · fat sour cream | · alcoholic drinks |
| · low-fat cottage cheese | Do not use vinegar in cooking |
| · hard cheese | sweet carbonated drinks |
| · soft cheese | |
| Legumes: peas, lentils | |
| vegetables: carrots, potatoes, cabbage, beets, tomatoes | |
| · fruits of all varieties | |
| · berries of all types | |
| Green vegetables are rich in iron | |
| · garden greens | |
| mineral water |
Prognosis for life with B12 deficiency anemia
Favorable prognosis; Poor prognosis
| with early treatment | with late therapy |
| · indicators in peripheral blood return to normal within 45 - 50 calendar days. | · severe anemia, which is difficult to treat. |
| · hemoglobin returns to normal within 30 - 60 calendar days. | · symptoms of damage to the centers of the nervous system, which does not recover. |
| · the B12 index is kept within the normative limits and anemia does not show its harmful effects on the body. | · the body does not accept medicinal B12, which is fraught with an anemic type of coma. |
| · with a genetic form of anemia, in most cases it is impossible to achieve a complete cure. Lifelong maintenance therapy in 70.0% of such patients. |
How to prepare for the test?
To eliminate errors in measurements that could affect research results, you should adhere to the following rules :
- Before donating blood from a vein, rest for 15 minutes so that your pulse returns to normal.
- The stomach must be empty, so it is forbidden to eat for 12 hours before the test.
- 12 hours before the test you should not smoke, drink alcohol or play sports.
- It is prohibited to take medications 1-2 days before the test. Otherwise, a decreased or increased level of vitamin B12 in the blood is possible. If stopping the medication is not possible, it is important to notify the laboratory staff.
- Children under five years of age must drink boiled water before donating blood (it is recommended to divide the intake into several portions of 170-200 ml). The liquid is drunk within half an hour.