A progressive surgical method of diagnosis and surgical intervention - laparoscopy, is successfully used for the treatment of the gastrointestinal tract, gynecological diseases, and in thoracic surgery (chest).
The range of applications of such operations on the organs of the digestive system includes:
- removal of part of the stomach (gastrectomy);
- excision of any part of the colon (colectomy);
- antireflux surgery (fundoplication);
- narrowing of the upper parts of the stomach (gastroplasty);
- laparoscopy of appendicitis (appendectomy).
The latter is used most often due to the widespread prevalence of the disease. Surgery is performed using a laparoscope - a device equipped with a video camera and a lighting component, as well as special surgical instruments. Removal of appendicitis occurs without opening the abdominal cavity, so laparoscopy is a minimally invasive surgical method.
Diagnostic laparotomy of the abdominal organs is most often performed when it is impossible to identify the pathology using hardware and laboratory methods.
The use of laparoscopy for the diagnosis and removal of appendicitis
Laparoscopy differs from classical surgery in that all manipulations are carried out through small holes - up to 1.5 cm. Performing the operation in the traditional way requires large incisions several centimeters long with layer-by-layer dissection of tissue.
Laparoscopy is used for both diagnosis and removal of the appendix. With this method, the doctor has the opportunity to thoroughly examine the condition of the internal organs and accurately determine the location of the inflammation.
Laparoscopy often allows you to combine diagnosis and surgery, which reduces the time to remove appendicitis.
Advantages and disadvantages of this method
Laparoscopy has a number of advantages over traditional surgery:
- rehabilitation takes much less time;
- less tissue damage than during abdominal surgery;
- aesthetic scars (small, invisible);
- faster recovery of working capacity;
- the patient experiences less pain, it goes away faster after the operation;
- bowel function is restored sooner;
- reducing the risk of complications and adhesions;
- reduction of hospital stay.
The method also has negative sides. These are mainly difficulties in the work of a doctor:
- depth perception is distorted;
- little space to manage tools;
- tactile sensations become dull;
- it is more difficult to control tools and your movements;
- There are a number of absolute and relative contraindications.
Why is laparoscopy prescribed?
This method is widely popular when performing gynecological operations. It is also used when other manipulations in the abdominal area are necessary.
Laparoscopy is performed in the following cases:
- acute appendicitis;
- a chronic form of the disease with pronounced symptoms and severe pain.
If inflammation has managed to cause peritonitis or an abscess, then abdominal surgery is indicated.
Who is laparoscopy indicated for?
There are several groups of patients for whom it is preferable to remove the appendix using the laparoscopic method:
- when it is unclear during diagnosis whether it is appendicitis or another disease; in this case, diagnostic laparoscopy becomes therapeutic;
- if a woman plans to become pregnant and have children in the future;
- with some concomitant diseases that increase the risk of complications (suppuration, formation of adhesions, etc.), for example, diabetes mellitus or obesity;
- children, as the risk of adhesions is reduced;
- the patient’s desire to avoid large, rough scars (only if there are no contraindications).
Indications
Acute and chronic forms of inflammation of the appendix are the main indicators when the appendix is removed. The condition is characterized by pronounced symptoms:
- Nausea and vomiting.
- Pain syndrome from the source.
- Increased body temperature.
In addition to inflammation of the appendix, indications for the use of surgery using a laporoscope are:
- Mucocele.
- Benign neoplasms, cysts, worms.
- Tumors caused by carcinoid lesions of organs.
The operation is possible in the following cases of concomitant diseases:
- Diagnostics does not confirm or exclude the inflammatory process. In this case, the operation turns from diagnostic to therapeutic.
- Women of childbearing age with unclear symptoms that do not allow a clear distinction between the inflamed appendix and gynecological disorders. Medical statistics note that almost half of patients with suspected appendicitis underwent an appendectomy without justification. In this case, the case of adhesions, which occurred as a complication, provoked infertility.
- Patients with diabetes and obesity, when a full cut will lead to a purulent complication.
- Childhood. Due to the minimally invasive method, the occurrence of adhesive disease is minimized.
Of course, when determining the method of operation, the patient's wishes are taken into account. In this case, you should take your choice seriously. If the hospital does not have a specialist who knows how to use a laparoscope, then it is better to refuse such a procedure.
If there are indications, then there are also contraindications for this surgical intervention:
- Kidney disease, liver dysfunction, cardiovascular disease.
- Pregnancy in the last months.
- Blood diseases leading to poor clotting.
Contraindications include pathologies located at the site of the intended operation:
- Increased density of inflammatory products, grouped inside and near the process.
- Adhesive processes.
- Accumulation of gases in the appendix. When trying to remove it, it can lead to a violation of the integrity of the appendix, touching nearby organs, provoking the development of peritonitis. Blood vessels and the walls of the intestinal tract are also at risk.
- Peritonitis in advanced form.
How to prepare for surgery
Usually, the vermiform appendix of the cecum must be removed urgently. The patient and doctors have a minimum of time. Preparation for the operation takes 2-3 hours.
Before an appendectomy, you will have to undergo some examinations: ultrasound of the abdominal cavity, general analysis of urine and blood, reaction to HIV, AIDS, hepatitis. If necessary, an ECG is performed.
Additional laboratory tests may be added depending on indications.
When the test results are received, the diagnosis is clarified and consent is given for surgical intervention, the patient begins to be prepared for surgery. This takes about 2 hours. During this time, the operating room is prepared, the patient is given antibiotics, sedatives and placed under general anesthesia.
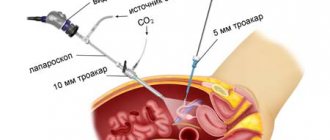
Then a small incision is made in the navel area and the stomach is filled with carbon dioxide through a needle. This is necessary so that the doctor can examine the internal organs, and also does not touch the abdominal wall during manipulations.
The surgeon conducts an examination and makes the final decision on the possibility of performing laparoscopy.
We receive sick leave
The procedure for issuing and filling out sick leave is regulated by the following regulations:
According to the law, a certificate of incapacity for work is issued by an employee of the health care institution where the patient was treated . After appendicitis, sick leave is issued by the attending physician upon discharge from the hospital.
How long does sick leave last after appendectomy? The duration of the certificate of incapacity for work is also determined by the attending physician on the basis of the law and depending on the general condition of the patient. It is calculated using the formula “length of hospital stay + rehabilitation period.”
Sick leave after appendicitis, how many days? The average number of days for rehabilitation varies:
- during laparoscopy – 5 – 7 days;
- for laparotomy - 10 - 15 days.
You may also be interested in the article “How much sick leave is given for chickenpox?”, which will surprise you, because with chickenpox the number of sick days is much greater.
It also happens that an employee of a medical institution made a mistake on the sick leave certificate, so we strongly recommend that you carefully check the document. If there is an inaccuracy in the name of the company, then read the article “Place of work on the sick leave certificate,” where you will learn how to correct this mistake.
How is the operation performed?
The removal of appendicitis itself using the laparoscopic method takes from 30 minutes to several hours. It all depends on the patient’s condition and the course of the disease.
When performing laparoscopy, general anesthesia is used, since substances that relax the muscles can be administered along with it. Local anesthesia is used only if there are contraindications to general anesthesia.
During the operation, the patient lies on his back, while the table tilts slightly to the left. Due to this, the intestinal loops and omentum are naturally removed, facilitating access to the appendix.
The skin is treated with an antiseptic.
A small incision is made near the navel, through which carbon dioxide is pumped into the abdominal area. Then, through the same hole, 1 trocar is inserted - a special surgical instrument that pierces the abdominal cavity, while maintaining its tightness.
With the help of a trocar, various manipulations are carried out inside the cavity without breaking the seal.
Then another incision is made in the left iliac region or below the navel in the middle. Through this hole, 2 trocars are inserted under the laparoscope. Through these 2 holes you can examine in detail the location and condition of the vermiform appendix.
After this, a 3rd incision is made and a 3rd trocar is inserted. If the location of the appendix is atypical or there are any obstructions (eg, adhesions), a 4th trocar may be needed. No large rough cuts are made. The holes for trocars look more like punctures.
If no contraindications to laparoscopy are found, then proceed with the operation. First, the appendix is fixed. Then a small incision is made through which a ligature is applied. After 1.5 cm, a second ligature is applied. Between them, the surgeon cuts off the appendix and carefully removes it without touching other internal organs.
The cecum is sutured. The laparoscopic operation ends with a control examination of the abdominal cavity and sanitation. All bleeding vessels are sutured. If there is pus or any signs of complications appear, then drainage is performed.
Carrying out
The procedure will be performed using specialized medical instruments:
- A device with a camera that allows you to examine the internal contents of the abdominal cavity - a laparoscope.
- The monitor on which camera data is displayed.
- A device for pumping carbon dioxide - an insufflator. Increases the volume inside and promotes better inspection of the surgical site.
- Laser to cut off an organ and immediately cauterize the cut-off site.
- A device for removing blood, pus and other things from the peritoneum - an irrigator-aspirator.
The process itself consists of the following manipulations:
- The appendix is fixed with a trocar, lifting it up to the inner wall of the cavity. Fixation is possible both at the mesentery and at the end.
- The film connecting the appendix and the large intestine is cut off. A hardware suture is applied.
- The entire appendix is cut off with a laser, and a suture is placed on the remainder. It is then hidden in the cecum and secured with staples and additional threads.
- The shoot is removed.
- Examine the abdominal cavity. Damaged blood vessels are being restored. Peritonitis and other forms of complications are corrected by drainage of the infiltrate.
- The incisions on the skin are sutured. The operation is completed.
What complications and consequences may there be?
During the operation, it may become clear that adhesions have arisen due to previous surgical interventions. This increases the risk of damage to other organs during laparoscopy.
If the appendectomy is performed correctly, then the risk of complications is minimal. They arise due to severe appendicitis, the general poor condition of the patient, the presence of concomitant diseases, and surgeon errors.
In general, the risk of complications after laparotomy is several times lower than with traditional appendectomy. To reduce their likelihood, a bandage can be used.
In rare cases, the following problems may occur:
- bleeding in the abdomen;
- development of peritonitis;
- the appearance of adhesions;
- development of abscesses;
- acute typhlitis;
- hypotension;
- the appearance of a hernia on the anterior wall of the abdominal cavity;
- development of secondary infection.
Unintended consequences
In case of technically faulty equipment or inadequate qualifications of medical personnel, in rare cases, the following negative consequences are possible after laparoscopy:
- burn of the cecum;
- an error when puncturing the abdominal cavity can lead to injury to healthy organs;
- labored breathing;
- concentration of gas bubbles under the skin (emphysema);
- internal bleeding;
- purulent infections of postoperative sutures;
- accidental damage to adjacent organs.
In some cases, a short-term decrease in blood pressure is possible.
Who is contraindicated for laparoscopy?
It is becoming increasingly popular and in some cases is even considered the preferred method for removing the appendix. However, there are a number of cases when such surgical intervention is impossible or undesirable.
Absolute contraindication:
- 3rd trimester of pregnancy;
- retroperitoneal phlegmon;
- intolerance to anesthesia;
- poor blood clotting;
- infiltrate;
- The appendix is not inflamed; another disease gives the clinical picture.
Relative contraindications:
- excess body weight;
- widespread peritonitis;
- previous operations;
- the presence of adhesions in the intestines.
Contraindications
The main indications for laparoscopy and removal of appendicitis using laparoscopy are symptoms of acute and chronic forms of appendicitis.
These conditions are evidenced by a clear clinical picture and changes detected by laboratory and instrumental examination methods. The list of contraindications is quite wide and includes both absolute and relative contraindications. The absolute ones include:
- Late pregnancy.
Traditionally, pregnancy has been considered an absolute contraindication for laparoscopy.
- Presence of contraindications to the use of anesthesia.
- Blood clotting disorders (hemophilia and other conditions with reduced blood clotting).
- No signs of inflammation of the appendix.
- Diffuse purulent inflammation in the retroperitoneal region.
- Appendicular infiltrate, representing a tightly fused appendix with intestinal loops.
Relative contraindications include the following situations:
- Increased body weight, making it difficult to access the abdominal cavity through laparoscopy.
- Previous diseases of the abdominal organs due to the risk of developing adhesions.
- Peritonitis, since the optimal treatment for it is wide laparotomy.
As a rule, recovery from appendicitis lasts at least 0.5 months.
The recovery period depends on how successfully the operation was performed, what method was used, how the body responded to the intervention, and the severity of the situation. After removal of purulent or gangrenous appendicitis, especially one that has turned into peritonitis, the rehabilitation period is longer, since there is a need to combat the infection that has developed, which includes long-term use of antibacterial drugs.
Today, appendectomy is performed by laparoscopy or abdominal surgery. Laparoscopic intervention is possible if the organ is inflamed, but tissue rupture has not yet occurred. This easy surgical treatment option provides for recovery after appendicitis removal within 2 weeks, less often 4.
Laparoscopic appendectomy is a minimally invasive surgical method that allows you to remove the inflamed appendix with minimal trauma. During the operation, the surgeon uses a laparoscope, or endoscope, which penetrates the abdominal cavity through a centimeter hole in the patient's abdomen.
A laparoscope is an optical tube made of metal with a video camera that contains 2 optical channels. One of them conducts light, which makes the area being operated easier to see. In the second, an image of the abdominal cavity is brought to the camera. The outer working diameter of the device is 10 mm.
In addition to the laparoscope, during surgery to remove appendicitis, the following are used:
- illuminator;
- clamps;
- forceps;
- electrocoagulator;
- insufflator
The image obtained from the laparoscope is fed to a video monitor and becomes available to the surgeons performing the operation
Laparoscopic appendectomy differs from classical surgery in that for all manipulations during surgical and diagnostic intervention it requires a small hole in the abdominal wall, approximately 1.5 cm. Classic surgery requires a larger incision that dissects the abdominal tissue layer by layer.
Laparoscopy is used both as a diagnostic method and as a means of removing the appendix. Diagnostic laparoscopy allows the doctor to know the exact location of the inflammation.
This significantly reduces the time of the diagnostic search and the operation itself to remove appendicitis if symptoms of chronic appendicitis were noticed. But when is laparoscopy used according to the clinic?
Laparoscopic appendectomy has absolute contraindications, these include the following conditions:
- severe coagulopathy;
- adhesions in the intestines;
- severe pathological processes occurring in the heart, liver, kidneys;
- history of abdominal surgery;
- abscess periappendicular process;
- peritonitis or the appearance of signs of its development;
- inability to use general anesthesia;
- detection of dense infiltrate in the area of the appendix
- processes accompanied by the formation of pus in the abdominal cavity.
Relative contraindications:
- old age;
- severe obesity;
- atypical location of the appendix;
- third trimester of pregnancy;
- disorders in the blood coagulation system;
- there is no idea of the real picture in the inflamed area (if it is not possible to make a diagnosis for a long time, laparoscopy is performed).
It has not been proven that pneumoperitoneum has a negative effect on the fetus, but minimally invasiveness during pregnancy is most preferable, since it allows you not to harm the baby and recover faster.
If blood clotting is impaired, serious bleeding may occur, but if appendicitis occurs, treatment is required in any case and it is desirable that it be less traumatic. The patient is prescribed replacement therapy, so blood loss is usually insignificant.
If you are overweight, the doctor may decide to perform laparoscopy, but only in cases where there are no aggravating circumstances. For obese patients, this technique is often chosen because abdominal surgery carries higher risks.
Removing appendicitis by laparoscopy has the following advantages:
- excellent cosmetic effect;
- minimal trauma;
- fast rehabilitation;
- lower incidence of complications;
- economic benefit associated with short hospitalization
- the ability to conduct a full examination of internal organs and perform additional operations without widening the incision.
Flaws:
- requires expensive equipment;
- staff need to be trained;
- inability to implement the technique for some concomitant pathologies.
Such surgical interventions, however, are not possible for everyone - in some cases there are contraindications.
Among the general contraindications are absolute:
- late pregnancy;
- intolerance to anesthesia;
- blood clotting disorder.
Relative contraindications include:
- overweight;
- previous operations.
According to local absolute contraindications, the following are undesirable:
- absence of inflammatory signs in the appendix;
- severe appendicular infiltrate;
- retroperitoneal phlegmon.
Local relative contraindications should not include:
- interintestinal adhesions;
- inflammation of the peritoneum.
Despite the fact that this technique is one of the safest and most gentle, it cannot be used for the following contraindications:
- problems with blood clotting;
- last trimester of pregnancy;
- inability to use general anesthesia;
- the patient has a history of abdominal surgery;
- the patient’s body weight is too large with a significant fat layer at the site of the incisions;
- there is no data on the actual inflammatory process, but if it is impossible for a long period of time to determine an accurate diagnosis, laparoscopy is still performed, but more as a diagnostic method;
- there are serious purulent processes outside the abdominal area;
- registration of dense infiltration in the affected area;
- the appearance of signs of possibly developing peritonitis or its actual development;
- the presence of adhesions on the intestines.
Abdominal surgery is a serious test for the patient’s health. In this regard, the laparoscopy method is several times safer and more productive. The patient does not require a long stay in a medical hospital, and there is no increased pain during the recovery period. The intestines are also restored several times faster, which relieves the patient of problems such as constipation or diarrhea. This in turn reduces the risk of dehydration or intoxication during the recovery period.
Typically, such an intervention is planned in advance, since in emergency cases, almost 100% of patients are operated on using the abdominal method. To carry out the intervention, the specialist will always require blood tests and ultrasound results. In the acute type of the disease, an x-ray examination is required, during which a specialist may detect additional difficulties in the form of accumulated hard feces and other disorders. Anamnesis must be checked for the contraindications described above. The operation is always performed strictly under general anesthesia.
If the operation is planned and is not acute, the patient is prepared for it as much as possible. An enema must be prescribed, which will eliminate accumulated feces and relieve increased gas formation, which can interfere with the normal work of the surgeon. Also, two hours before the start of surgery, the patient is given therapeutic doses of antibiotics and sedatives. If the patient's condition quickly deteriorates, he is given doses of antibiotics and immediately sent to the operating table.
The operation itself consists of several mandatory steps:
- the surgeon carefully examines the patient’s abdominal cavity for external and other injuries;
- then the sore spot is treated with an antiseptic drug and an incision is made;
- for the convenience of the specialist and the safety of the patient, two upper and two lower incisions are made on both sides of the abdomen;
- the specialist inserts a special tube with a camera into the incision, with the help of which he once again carefully examines the abdominal cavity, but this time inside the patient;
- Using special forceps, the surgeon exposes and slightly pulls the appendix towards the incisions;
- the next stage of the operation is excision of the mesenteric part of the intestine;
- as soon as the mesentery is excised, special forceps grasp the inflamed process and remove it;
- simultaneously with its removal, the specialist sanitizes the cut so that the inflammatory process does not advance through the digestive system;
- Only after antiseptic treatment is the appendix removed through the incisions;
- as soon as it is removed, complete sanitation of the peritoneum is also carried out, and if peritonitis develops, drainage is installed;
- after removal, the doctor examines the wound again so that there is no pus or working tools left in it;
- The last stage of treatment is suturing and external treatment of the incisions with an antiseptic.
| By-effect | Frequency of occurrence |
| Perforation of appendicitis due to clamp weakness | Rarely |
| Perforation of the cecum | Rarely |
| Poor closure of the duct of the artery leading to appendicitis, which provokes bleeding | Sometimes |
| Poor sanitation of incisions, sutures and inflamed areas | Sometimes |
| Formation of small hematomas on the abdominal wall | Often |
| Necrotic processes on the remaining part of the appendicitis | Sometimes |
| Hernia formation on incisions | Rarely |
| Development of peritonitis after surgery | Rarely |
| Massive bleeding due to arterial damage | Rarely |
Recovery after surgery
The recovery period after laparoscopy takes little time. The period of complete restriction of physical activity is limited to several hours. The next day, the patient is allowed to get out of bed and move around, for example, to independently walk to the office where the dressing is done.
But you shouldn’t get too carried away: it will be possible to give the body a full load only after 2 months, when the circumcised intestines have healed. Restrictions on carrying heavy objects are especially strict.
How long does it take to be discharged after appendix removal? Patients are sent home 3-7 days after surgery. The drainage is removed the next day. While in the hospital, infusion treatment continues and a course of antibiotics is administered.
In the first few days, pain is possible after laparoscopy in the area of punctures and suturing. Therefore, the patient will be given anesthetics.
Sutures are removed after 7-10 days. This is done in the clinic or in the department where the operation was performed. Many people are concerned about whether it hurts to remove stitches. Due to the fact that they are small, the procedure is almost unnoticeable.
It is possible to use self-absorbable threads. Then you won't have to remove the stitches.
What can you eat after surgery? On the first day after laparoscopy, the patient will be given mainly drinks and liquid food. In the next few days, gentle nutrition is indicated. However, in just a week you will be able to switch to the regular menu.
But this does not apply to alcohol !
You can drink alcohol no earlier than 1.5-2 months after appendectomy. It is better to start with light drinks in small quantities, for example, 100 ml of red wine will be enough for the first time. Alcohol must be of high quality.
Rehabilitation period
Immediately after the operation, the patient is transferred to the intensive care unit, where his condition is monitored throughout the day. At this time, the operated patient is given antibiotics to prevent inflammation, glucose and vitamin solutions to restore the body, as well as painkillers.
On the second day, the patient is transferred to the general ward. Sutures after laparoscopy are removed on day 3, after laparotomy - on day 5, after which the patient is discharged.
In some cases, the operated patient experiences a temporary increase in body temperature as a reaction of the body to the intervention. Temperature may rise sporadically throughout the entire rehabilitation period.
The duration of rehabilitation depends on the preoperative condition of the person, his age and compliance with the recommendations of the attending physician. Typically, full recovery takes from 10 days to 4 weeks. Children and the elderly take the longest to recover.
Particular attention should be paid to a diet that excludes foods whose consumption leads to intestinal dysfunction - increased gas formation, constipation, diarrhea, etc. A balanced, high-calorie diet is preferable, necessarily including fresh vegetables and complete protein. These products will replenish the body's energy costs for recovery and speed up rehabilitation.
During this period, it is recommended to exclude heavy physical activity, including sports. It is also necessary to limit visits to the sauna and solarium. The suture can be treated with anti-scar ointments, but not earlier than 2-4 months after the operation. We also advise you to read the article “Violation of hospital regulations”, from which you will learn what the consequences of non-compliance with medical orders are.
Types of appendectomy
Several methods of appendectomy are used in surgery.
The most common of them, as well as their advantages and disadvantages, are listed in the table below:
| Method | Essence of the method | Advantages | Flaws |
| Laparoscopy | Trocars, hollow tubes containing a surgical instrument, are inserted into the abdominal cavity. |
|
|
| Access according to Volkovich - Dyakonov | The tissue incision is made obliquely, parallel to the inguinal ligament. |
|
|
| Pararectal laparotomy according to Lenander | The incision is made in the longitudinal direction, at a distance of 1 cm from the right rectus muscle. |
|
|
| Transverse laparotomy according to Winkelmann | The incision is made in the transverse direction at the level of the bispinal line, tangent to the wings of the ilium. |
|
|
Laparoscopy is currently the most promising surgical method not only for appendicitis, but also for other diseases.
Meals after discharge
At home, you also need to stick to a diet. Usually, upon discharge, the doctor gives recommendations on dietary habits. They definitely need to be followed. This diet should be followed for 1-2 months.
Prohibited Products
The most important thing is to exclude foods that can cause increased gas formation. These are legumes, cabbage, many vegetables and fruits, carbonated drinks. It is also forbidden to eat food that activates gastric secretion. A large number of enzymes irritate the intestinal mucosa and slow down healing. These are strong broths, seasonings, salt, acids, food rich in essential oils.
Coarse fiber, which can cause gas formation, is prohibited. These are legumes, all types of cabbage, turnips, radishes, corn. Refractory fats, margarine, and lard should be avoided. Any fatty food is difficult to digest, creating a load on the intestines. You need to avoid drinks with a tonic effect. A strict ban on all canned food, semi-finished products and products with E-additives.
There are many foods in the diet after appendectomy that are prohibited:
- rolls, black bread;
- fatty meat, offal;
- rich fatty broth;
- sausages, ham;
- marinades, pickles;
- sweets, confectionery;
- sweet soda;
- fatty dairy products;
- millet, pearl barley;
- some fruits;
- alcohol.
Authorized Products
Despite the large number of prohibited foods, the diet after appendicitis in adults is quite varied. From the second week, the diet expands. Food should contain all the necessary proteins and carbohydrates, as well as vitamins. It is important that the food is easily digestible. There are many permitted products:
- dried bread, crackers;
- lean fish, white chicken meat, in the form of soufflés, meatballs, steam cutlets;
- slimy porridge with water or half-and-half milk;
- pureed vegetable soups;
- pureed, stewed or baked vegetables;
- soft-boiled eggs or omelet;
- low-fat cottage cheese and yogurt;
- berry jelly or compotes;
- honey;
- baked apples;
- green tea, herbal decoctions.
Menu
All the time when you are on a diet, you need to eat fractionally. The diet consists of main meals and 2-3 snacks. You should not overeat so that food is well digested; it is important to boil or grind it. Usually the doctor creates the menu individually. But you can use a ready-made diet menu after appendicitis in adults by day.
| Days | Breakfast | Snack | Dinner | Afternoon snack | Dinner | For the night |
| 1 | Slimy oatmeal, tea with milk | Rose hip decoction | Soup with chicken meatballs, rice porridge, sugar-free jelly | Blueberry compote | Buckwheat porridge, soft-boiled egg | Natural low-fat yogurt |
| 2 | Mashed cottage cheese, kefir | Dried fruits | Chicken broth, vegetable casserole, boiled egg, rosehip infusion | Yogurt | White meat chicken soufflé with rice, tea with milk | Currant jelly |
| 3 | Omelette, chamomile decoction | Baked apples | Puree vegetable soup, steamed chicken cutlets, compote | Kissel, cookies | Puree cottage cheese, yogurt | Ryazhenka |
| 4 | Rice porridge, compote | Tea, biscuits | Chicken broth, steamed meatballs with rice, tea | Baked apple | Chicken soufflé, mashed potatoes, compote | Low-fat kefir |
| 5 | Buckwheat porridge, egg, tea | Curd soufflé | Puree rice soup, steam cutlets, rosehip infusion | Natural yogurt | Potato casserole with chicken, dried fruit compote | Cherry jelly |
| 6 | Curd casserole, fermented baked milk | Apple | Chicken broth, steamed cutlets with vegetable stew, pumpkin juice | Chamomile decoction, biscuits | Buckwheat porridge, steamed fish cutlets, jelly | Yogurt |
| 7 | Semolina porridge with milk, tea | Fruit jelly | Vegetable puree soup, boiled meat, buckwheat, tea | Kissel, cracker | Chicken soufflé, vegetable stew, compote | Kefir |
Recipes
All foods consumed after surgery should not put stress on the intestines. But it is important that the food is also tasty. Then the food will be better absorbed. There are several simple recipes for preparing dietary dishes.
- Steamed meatballs with rice are made from beef. It is scrolled in a meat grinder three times. The cooked rice is washed well, then mixed with minced meat and seasoned with salt. Form small meatballs and steam them.
- It is also better to steam fish cutlets. Chop the fillet, add an egg and finely chopped onion. It is better to make them in a double boiler.
- Meat soufflé can be made from chicken or veal. The meat is boiled, minced, and mixed with the yolk. Then add the whipped egg white. Place the mixture into molds and bake in the oven.
Physical activity in the postoperative period
A sedentary lifestyle during the rehabilitation process is no less dangerous than high physical activity. It can cause the formation of adhesions, poor circulation, or the development of muscle atrophy. In this regard, almost immediately after the operation, in agreement with the doctor, in a supine position, it is recommended to perform a special complex of exercise therapy.
In the first two months, physical activity should be limited to daily walking and therapeutic exercises. During this period, it is prohibited to carry or lift weights weighing more than 3 kg. After 14 days after surgery, if there are no contraindications, you are allowed to resume sexual activity. When the postoperative scar has completely healed, a visit to the pool is recommended.
How dangerous is the operation?
The incidence of postoperative complications is 5-9%. However, if we compare it with the mortality rate from appendicitis itself (in the 19th century, for example, it accounted for 40% of patients), then this is an insignificant figure. The cause of death with untreated appendicitis in most cases is diffuse peritonitis (inflammation of the peritoneum) and acute intestinal obstruction.
Complications mainly occur in those patients who sought medical help late or were diagnosed late. Most often they consist of the formation of abscesses in various areas of the abdominal cavity, which is associated with insufficiently complete removal of the affected tissue during surgery. Other types of complications are listed below.
Acute appendicitis
Acute appendicitis is an inflammatory disease that affects the appendix (vermiform appendix) and can develop at any age. As a rule, the disease begins with an acute painful attack in the right lower abdomen. In this case, the inflammatory process first occurs in the mucous membrane of the appendix, and then it spreads to all other layers, which leads to the appearance of all clinical symptoms.
Inflammation itself is not dangerous, however, removal of appendicitis is an important measure to prevent a serious complication - peritonitis, characterized by the spread of inflammation to the abdominal wall. The sooner the appendix that has changed as a result of the inflammatory process is removed, the better the prognosis for recovery after treatment.
Moreover, if a person has had the appendix removed at least once, the disease will never recur due to its absence. If acute pain appears in the lower right half of the abdomen, you should immediately consult your doctor or call an ambulance. Acute appendicitis can occur in a fulminant form, which is characterized by the rapid development of peritonitis.