X-ray of the chest organs in a direct projection.
You can see the accumulation of air under the diaphragm domes. Not to be confused with Fluoroscopy.
X-ray
(from
X-ray
(surname of the inventor) + Greek gráphō, I write) - the study of the internal structure of objects that are projected using X-rays onto a special film or paper. Most often, the term refers to a non-invasive medical study based on obtaining a summary projection image of the anatomical structures of the body by passing X-rays through them and recording the degree of attenuation of the X-ray radiation.
Content
- 1. History
- 2 Application 2.1 In medicine
- 2.2 In engineering and technology
- 2.3 In forensics
- 2.4 In restoration and examination of artistic values
- 3.1 Method of recording X-ray radiation
- 4.1 Analogue 4.1.1 Digital
History[ | ]
X-ray imaging, 19th century
The history of radiology begins in 1895, when Wilhelm Conrad Roentgen first recorded the darkening of a photographic plate under the influence of x-rays. He also discovered that when X-rays pass through the tissues of the hand, an image of the bone skeleton is formed on a photographic plate. This discovery became the world's first medical imaging method; before this, it was impossible to obtain intravital, non-invasive images of organs and tissues. Radiography spread very quickly throughout the world. In 1896, the first X-ray was taken in Russia.[1]
In 1918, the first X-ray clinic was created in Russia. Radiography is used to diagnose an increasing number of diseases. Lung radiography is actively developing. In 1921, the first X-ray dental office was opened in Petrograd. Research is being actively carried out and X-ray machines are being improved. The Soviet government is allocating funds to launch the production of X-ray equipment in Russia. Radiology and equipment production are reaching a global level.[2]
Nowadays, chest X-rays are often used to diagnose diseases caused by lung infections. However, this method was not very effective in detecting the early stages of viral pneumonia caused by COVID-19.
American researchers led by a professor at Ohio State University studied x-rays of 630 patients with confirmed coronavirus and severe symptoms. In 89 percent of cases, no abnormalities were noticeable on the X-ray, or they were minor. The practice of doctors at City Clinical Hospital No. 40 in the village of Kommunarka, who were the first to bear the brunt of the pandemic in Russia, also confirmed these conclusions. However, in later stages, radiography can provide accurate and high-quality results. That is why in the current situation, portable devices that can be used in the wards of patients in serious condition are especially relevant[3].
Currently, radiography remains the main method for diagnosing lesions of the osteoarticular system. Plays an important role in lung examination, especially as a screening method. Contrast radiography methods make it possible to assess the state of the internal relief of hollow organs, the prevalence of fistulous tracts, etc.
On July 13, 2020, New Zealand scientists presented in Geneva an X-ray machine that is capable of taking three-dimensional color images[4].
X-ray of the hip joint
Radiography allows specialists to see deviations from the norm in the formation of hip joints in children and pathologies of joint development. The main defect of the hip joints that can be detected using radiography is joint dysplasia.
Normal and displaced hip
Without this examination, diagnosing dysplasia is difficult, since only the results of an external examination do not provide complete confidence in the correctness of the diagnosis.
Dysplasia or congenital hip dislocation is a pathology of the development of pelvic joints in the fetus. This happens because all the components of the joint during the development of the fetus either slowed down their development or stopped developing altogether.
Application[ | ]
In medicine[ | ]
Radiography is used for diagnosis: X-ray examination (hereinafter referred to as X-ray) of organs allows us to clarify the shape of these organs, their position, tone, peristalsis, and the state of the relief of the mucous membrane.
- RI of the stomach and duodenum (duodenography) is important for recognizing gastritis, ulcerative lesions and tumors.
- RI of the gallbladder (cholecystography) and biliary tract (cholegraphy) is carried out to assess the contours, size, lumen of the intra- and extrahepatic bile ducts, the presence or absence of stones, and clarify the concentration and contractile functions of the gallbladder.
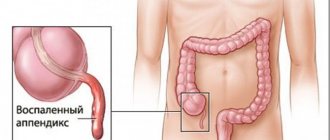
- RI of the colon (irrigoscopy) is used to identify tumors, polyps, diverticula and intestinal obstruction.
- chest x-ray – infectious, tumor and other diseases,
- spine - degenerative-dystrophic (osteochondrosis, spondylosis, curvature), infectious and inflammatory (various types of spondylitis), tumor diseases.
- various parts of the peripheral skeleton - for various traumatic (fractures, dislocations), infectious and tumor changes.
- abdominal cavity - organ perforation, kidney function (excretory urography) and other changes.
- Metrosalpingography is a contrast X-ray examination of the uterine cavity and the patency of the fallopian tubes.
- teeth - orthopantomography
- RI of the breast - mammography
In engineering and technology[ | ]
Radiography is one of the most important types of non-destructive testing. Used during production and operation to control:
- Castings and forgings for the presence of cracks, gas and shrinkage cavities;
- Welding seams for the presence of lack of penetration, thermal and mechanical cracks, slag inclusions, cavities;
- Load-bearing structures, shafts, axles, housings for the presence of internal cracks and fractures;
- Non-dismountable or difficult to disassemble machines and mechanisms for the correct relative position of the elements of their integrity and the presence of the necessary clearances;
- Reinforced concrete for the presence of voids, displacement cracks or destruction of reinforcement and embedded elements;
- Metallurgical furnaces during operation lead to the formation of deposits on internal surfaces;
- Various metal parts to detect welds, holes and cavities filled with other materials that were not intended by the design or intentionally disguised. In particular, to identify the fact that the marking containing the VIN on the car body has been replaced.
In criminology[ | ]
- Research into the internal structure of objects;
- Examination of car or weapon parts for changes in markings (in recent years it has been replaced by other methods of analysis);
- Forensic research.
In restoration and examination of artistic values[ | ]
- Research into the artist’s “handwriting”;
- Research of traces of canvas restoration;
- Exploring hidden images (when reusing the canvas);
Hip dysplasia
With hip dysplasia, the joints themselves significantly change their shape, and their structures also change in size. In this case, the glenoid cavity may become flatter, the ligaments become too elastic, so the articular capsule does not hold the head of the tibia in the acetabulum well. So, with any change in the position of the femur, its head “pops out” from the socket, and this is how subluxation or dislocation occurs.
The correct location of the hip joints is determined by such a concept as the neck-diaphyseal angle (or NDA). The SDF is formed by the intersection of a straight line dividing the diaphysis in half and a straight line connecting the conditional centers of the head and cervical part of the femur bone.
Measuring the neck-shaft angle
On an x-ray, doctors measure the resulting angles. The normal position of the joint relative to the acetabular notch is when an imaginary straight line passing through the head and cervical part of the femoral bone divides the segment that connects the edges of the acetabular notch in half, and the angle obtained at the intersection of these lines is almost straight.
Different types of hip dysplasia have different angles of the femur relative to the acetabulum. When there are such deviations of the NDS from the norm in an infant, we can talk about abnormal development of the upper part of the tibia.
Determination of dislocation in a child
There are various methods that can be used to determine the presence (or absence) of hip dislocation in an infant.
It is normal if in children:
- legs are the same length and located symmetrically relative to each other;
- if the folds of the skin located under the buttocks of the baby are symmetrical;
- muscle tone in the legs is within acceptable normal limits;
- the correct ratio of active and passive leg movements in infants.
If parents notice any deviations from the norm in their baby, then this is a reason to contact a pediatric surgeon. To more accurately determine congenital hip dislocation, the doctor will definitely order an x-ray of the hip joint. True, many parents believe that it is harmful for a child in his first year of life to undergo such a procedure.
However, the level of radiation that the baby receives during an x-ray examination is negligible and will not harm the baby. But untimely treatment of dysplasia (especially in girls) can lead to irreversible consequences. The fact is that in children, bone tissue is just beginning to form; basically, the baby’s bone skeleton consists of cartilaginous tissue, which is softer. Such tissues can take any shape, which is why it is so important to change the incorrect position of the bones and joints of the pelvis and legs in a timely manner.
Receiving an image[ | ]
Method of recording x-ray radiation[ | ]
Obtaining an image is based on the attenuation of X-ray radiation as it passes through various tissues and its subsequent recording on X-ray sensitive film. As a result of passing through formations of different densities and compositions, the radiation beam is scattered and decelerated, and therefore an image of varying degrees of intensity is formed on the film. As a result, the film produces an averaged, summation image of all tissues (shadow). It follows from this that in order to obtain an adequate x-ray, it is necessary to study radiologically heterogeneous formations.[5]
In modern X-ray machines, the output radiation can be recorded on a special film cassette or on an electronic matrix. Devices with an electronic sensitive matrix are much more expensive than analog devices. In this case, films are printed only when necessary, and the diagnostic image is displayed on the monitor and, in some systems, stored in the database along with other patient data.
Principles of radiography[ | ]
When performing diagnostic radiography, it is advisable to take pictures in at least two projections. This is due to the fact that an x-ray is a flat image of a three-dimensional object. And as a consequence, the localization of the detected pathological focus can be established only using 2 projections.
Image acquisition technique[ | ]
The quality of the resulting X-ray image is determined by 3 main parameters: the voltage applied to the X-ray tube, the current strength and exposure (duration of the X-ray radiation). Depending on the anatomical formations being studied and the weight and dimensions of the patient, these parameters can vary significantly. There are average values for different organs and tissues, but it should be noted that actual values will vary depending on the machine used and the patient undergoing the x-ray. An individual table of values is compiled for each device. These values are not absolute and are adjusted as the study progresses. The quality of the images taken largely depends on the ability of the radiographer to adequately adapt the table of average values to a specific patient.[6] To reduce the dynamic blur of images caused by non-absolute immobility of the organ under study or the patient himself, the required exposure should be created with a short shutter speed and high peak power of the X-ray tube.
Stages of implementation
Preparing for a hip x-ray
X-ray of the femur does not require the patient to follow strict preparatory procedures. But in order for the results to be as accurate as possible, it is worth paying attention to important points. Since the location of the left or right thigh is located near the rectum, before the study it is worth clearing it of feces using a laxative or enema. It is important to eliminate excess gases; for this purpose, special medications are prescribed, for example, Espumisan. If contrast is used, it is important to pre-test for an allergic response. If the reaction is negative, the procedure can be carried out.
Methodology
In order for the x-ray anatomy of the hip joint to show the extent of the damage, a lateral photograph is taken in a direct projection, capturing the lumbar and thoracic spine. To get a more accurate picture, images are taken in two projections. To obtain a direct image, the patient is placed on his back with his legs in a straight line with his feet turned inward. If it is necessary to obtain an image of a flexor joint, radiography is performed in a sitting position, the bending line is determined by the doctor. If it is necessary to administer contrast, 3-5 minutes before. Before the procedure, an injection is given, then the doctor takes pictures.
If it is indicated to take an x-ray of the hip joint in an infant, the baby is laid down with the legs straightened along a straight line. It is important that the limbs do not bend, because in this case the study does not always show the full picture of the disorders. So that the child does not have fear, and body movements do not distort the data, it is recommended to administer a sleeping pill before the examination.
Decoding
If the preparation for the study was correct, based on the images obtained, the doctor will be able to make a preliminary diagnosis. Normally, the resulting images should not show any pathological shadows if the person is healthy and the outlines of the bones are clear. Each pathology is different, as can be seen in the picture:
- Bone fragments are visualized during a fracture.
- If there is a displacement of the joints, then the patient has a dislocation.
- When bone density decreases, osteoporosis can be suspected.
- Pathological development of the femoral head indicates dysplasia.
- Neoplasms that are visible on images as dark lesions indicate tumor diseases.
Return to contents
Results in a child
Decoding an X-ray for a baby has its own peculiarities. The results are interpreted by a pediatric orthopedist or traumatologist. Due to the cartilaginous structure of the head of the hip bone, which is poorly visible on the resulting image, the doctor will not be able to determine the pathology, so the Hilgenreiner technique is used. The inclination of the roof of the acetabulum is assessed, the angle of which is different for each age. If the roof slopes at a large angle, this indicates dysplasia of varying severity.
If the pathology of the hip joint in a child is congenital, and urgent diagnosis is required, and radiography is contraindicated, an alternative method of examination is ultrasound diagnostics. This is a frequently prescribed and gentle examination method that can be performed at any age, as it has no contraindications.
Recording an image[ | ]
In Russia, the most common way to record an X-ray image is to record it on X-ray sensitive film and then develop it. Currently, there are also systems that provide digital recording of data. In most developed countries, this method has already replaced the analog one. In Russia, due to the high cost and complexity of manufacturing, this type of equipment is inferior in prevalence to analog.
Analog[ | ]
There are the following options for obtaining images using X-ray film.
One of the previously used methods for obtaining usable density images is overexposure followed by underexposure, made during visual inspection. Currently, this method is considered obsolete and is not widely used in the world.
Another way is adequate exposure (which is more difficult) and full development. With the first method, the X-ray load on the patient is overestimated, but with the second, it may become necessary to take repeated photographs. The advent of on-screen preview of a computerized X-ray machine with a digital matrix and automatic developing machines reduces the need and possibility of using the first method.
It should also be noted that the quality of the image is reduced by dynamic blur. That is, the blurring of the image is associated with the movement of the patient during irradiation. A certain problem is secondary radiation; it is formed as a result of the reflection of X-ray radiation from various objects. To filter scattered radiation, filtration gratings are used, consisting of alternating strips of X-ray transparent and X-ray opaque material. This filter filters out secondary radiation, but it also weakens the central beam, which requires a large dose of radiation to obtain an adequate image. The need to use filter grids is decided depending on the size of the patient and the organ being x-rayed.[7]
Many modern X-ray films have very low intrinsic X-ray sensitivity and are designed for use with intensifying fluorescent screens that emit blue or green visible light when irradiated with X-rays. Such screens, along with the film, are placed in a cassette, which, after the image is taken, is removed from the X-ray machine and then the film is developed. Film development can be done in several ways.
- Fully automatic when a cassette is inserted into the machine, after which the developing machine removes the film, develops it, dries it and refills it with a new one.
- Semi-automatically, when the film is removed and loaded manually, and the developing machine only develops and dries the film.
- Completely manually, when development takes place in tanks, the film is removed, refilled, and developed by an X-ray technician.
For X-ray image analysis, an analog X-ray image is recorded on an illuminating device with a bright screen - a negatoscope.
Digital[ | ]
Resolution[ | ]
Resolution reaches 0.5 mm (1 pair of lines per millimeter corresponds to 2 pixels/mm).
One of the highest film resolutions is considered to be “26 pairs of lines per mm,” which approximately corresponds to a resolution of 0.02 mm.
Preparing the patient for x-ray examination[ | ]
Special preparation of patients for x-ray examination is generally not required, however, the following preparation methods are available for examination of the digestive organs:
- Previously, special diets were carried out, foods that contributed to flatulence were excluded from the diet, and a cleansing enema was performed, but now it is generally accepted that RI of the stomach and duodenum of patients with normal intestinal function does not require any preparation. However, in case of severe flatulence and persistent constipation, a cleansing enema is performed 2 hours before the test. If there is a large amount of liquid, mucus, or food debris in the patient’s stomach, gastric lavage is performed 3 hours before the test.
- Before cholecystography, the possibility of flatulence is also excluded and a radiopaque iodine-containing drug is used (cholevid, iopagnost 1 g per 20 kg of live weight). The drug enters the liver and accumulates in the gallbladder. To determine the contractility of the gallbladder, the patient is also given a choleretic agent - 2 raw egg yolks or 20 g of sorbitol.
- Before cholegraphy, the patient is injected intravenously with a contrast agent (bilignost, bilitrast, etc.), which contrasts the bile ducts.
- Before irrigography, it is carried out using a contrast enema (BaSO4 at the rate of 400 g per 1600 ml of water). On the eve of the study, the patient is given 30 g of castor oil, and in the evening a cleansing enema is given. The patient does not have dinner, the next day a light breakfast, two cleansing enemas, a contrast enema.
Preparation
If an emergency arises, no special preparation is required before performing a routine examination without contrast.
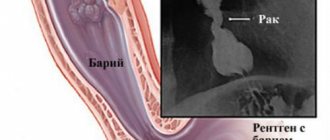
During fluoroscopy with contrast, the patient is given a glass of warm water in which the contrast agent, barium sulfate, is diluted.
After a minute, the liquid completely enters the stomach and a standard photo is taken in a standing position. It is repeated after a few minutes to visualize the passage of fluid into the duodenum.
With double contrast, a solution of barium sulfate is used , which is given to the patient through a special tube with holes. Through them, air enters the digestive tract, which increases the information content of the technique. In addition to barium, 2 tablespoons of an astringent (“Almagel”), 2 g of sodium citrate and 10 drops of a 96% alcohol solution are added to the solution. The volume of contrast for an adult patient is one third of a glass.
Help During a routine x-ray examination of the abdominal organs, you must refrain from eating any food 9-10 hours before. This significantly increases the information content of the study. Fluid intake should be limited one hour before the procedure.
Special preparation is required for elderly patients who often suffer from chronic digestive problems (increased gas production, frequent constipation). They are prescribed a special diet 2-3 days in advance. Products that may contribute to fecal stagnation are excluded from it. In this case, fluoroscopy will show pathologies of the esophagus as accurately as possible.
In children
The last feeding of infants should be 3 hours before the start of the procedure. Next, as a rule, they should skip meals.
For older children, the food retention time is 4 hours. Moreover, if the child complains of hunger or cries, then he can be given a small amount of water to drink.
Psychological preparation for research is important. It is necessary to convincingly tell that this procedure is absolutely painless and will not cause any discomfort. It should be remembered that children are often sensitive to the emotions of their parents, and therefore you need to remain calm and have a positive attitude.
In pregnant women
Important X-ray examinations are not performed in pregnant women due to the risk of harmful effects of ionizing radiation on the fetus.
Taking medications
X-rays of the stomach do not require discontinuation of medications that the patient is taking due to other somatic diseases.
If contrast is required, the patient’s preparation is most thorough: before the procedure, the digestive tract must be cleaned as much as possible.
Therefore, in addition to the diet, they are given a laxative based on macrogol (Fortrans, Endofalk) orally 24 hours before. Additionally, on the day of the study, a cleansing enema may be prescribed. Sometimes sorbents are prescribed - drugs that absorb gases and various substances from the cavity of the digestive tract (Enterosgel, Smecta, Polysorb).
Please note: During fluoroscopy of the stomach and duodenum, antispasmodics (papaverine, drotaverine, mebeverine) are discontinued 24 hours before.
Disadvantages of radiography[ | ]
- The static nature of the image makes it difficult to assess organ function.
- The presence of ionizing radiation that can have a harmful effect on the patient.
- The information content of classical radiography is significantly lower than such modern medical imaging methods as MRI, etc. Conventional X-ray images reflect the projection layering of complex anatomical structures, that is, their summation X-ray shadow, in contrast to the layer-by-layer series of images obtained by modern tomographic methods.
- Without the use of contrast agents, radiography is not informative enough to analyze changes in soft tissues that differ little in density (for example, when studying the abdominal organs).
Notes[ | ]
- History of radiology (Russian) (inaccessible link). Retrieved September 23, 2009. Archived January 22, 2012.
- History of radiology in Russia (Russian) (inaccessible link). Retrieved September 23, 2009. Archived April 17, 2012.
- Medical diagnostic technologies: what new we learned during the pandemic (unspecified)
.
Naked Science
(August 5, 2020). Retrieved August 31, 2020. - Scientists were able to obtain three-dimensional color X-ray images for the first time (unspecified)
. TASS (July 13, 2018). Retrieved July 15, 2020. - Kishkovsky A.N., Tyutin L.A., Esinovskaya G.N.
Atlas of placements for X-ray examinations. - Leningrad: Medicine, 1987. - P. 6-7. — 520 s. - (04567). - Kishkovsky A.N., Tyutin L.A., Esinovskaya G.N.
Atlas of placements for X-ray examinations. - Leningrad: Medicine, 1987. - P. 32-46. — 520 s. - Kishkovsky A.N., Tyutin L.A., Esinovskaya G.N.
Atlas of placements for X-ray examinations. - Leningrad: Medicine, 1987. - P. 21-24. — 520 s.