Gastrointestinal cancer can be detected in the early stages of development, but only with the use of the CA 72-4 tumor marker. This is a method that shows the presence of cancer before symptoms appear. One of the first on the list of cancers of the gastrointestinal tract is stomach cancer. Timely diagnosis of oncological development is quite difficult, so the disease is often detected during the later stages of progression. In this case, the likelihood of successful cancer treatment is minimized.
Analysis of the antigen, which is produced in large quantities in oncology, allows not only to determine the stage of the disease, but also to identify the spread of metastases to tissue and blood, as well as to other organs and structures (for example, in pancreatic cancer with metastases to the bones). If an increase in antigen levels is detected, the doctor issues an order regarding what tests still need to be taken to confirm the patient’s diagnosis. To understand the indications for analysis and interpretation of research results, it is worth familiarizing yourself in more detail with all aspects of this diagnostic method. Diagnosis and treatment of oncology should be carried out exclusively in a specialized medical institution.
Tumor marker Ca 72 4 establishment of indicators and reasons for deviation from the norm
The organs of the digestive system make it clear about the development of pathology before other systems. This allows you to identify the problem in the early stages, determine the diagnosis and prescribe effective treatment.
Indicators of tumor development in the stomach
Since stomach cancer is often asymptomatic, it is difficult to detect it in the early stages. Often the diagnosis is made after the body is affected by metastases and the prescribed treatment is ineffective. Tumor marker CA 72-4 is an indicator that helps to identify oncology even before symptoms of the disease appear.
What do the indicators mean?
As cancer develops, tissue changes occur. In this case, the neoplasm may differ in its morphology (structure). As a tumor develops, it produces specific substances called tumor markers. Evidence that an oncological process is developing in the patient’s body is the presence of an antigen in the blood.
Analysis for specific substances is not only a method for identifying malignant neoplasms, but also allows you to dynamically monitor the effectiveness of the prescribed course of therapy.
Today, about two hundred substances are known that are released into the blood by different types of neoplasms, however, only a few of them are of diagnostic value.
Stomach cancer, what markers are used in diagnosis?
The most informative marker for diagnosing diseases of the stomach and gastrointestinal tract is the 72-4 ca tumor marker. This antigen is a complex of protein and oligosugars.
Against the background of an inflammatory disease occurring in the patient’s body, there may be an increase in tumor markers in the blood. Such nonspecific growth is often not associated with cancer problems and is not a cause for concern.
Important
The course of any oncological process does not always manifest itself clinically, but laboratory testing allows pathology to be detected in the early stages.
Indicators differ depending on the type of tissue where the tumor develops. Thus, tumor marker 72-4 may increase:
- in 40 percent of cases – with oncology of the gastrointestinal tract and stomach;
- in 36 percent of cases – with the development of tumors in the lungs;
- in 24 percent of cases - with ovarian cancer.
If the tumor marker ca 72-4 is elevated, this may be evidence of diseases such as gastritis, cirrhosis, pancreatitis, gastric and duodenal ulcers.
The difference between the CA 242 tumor marker and other tumor markers during diagnosis
It is noted that the expression of the CA 242 epitope occurs, as does the expression of CA 19-9 - Sialyl Lewis (SLea) on the same mucin apoprotein. The expression of CA 242 is higher than CA 19-9, so the protein is considered more specific. When diagnosing pancreatic cancer and chronic pancreatitis, CA 242 will be 1.4 times more sensitive than CA 19-9.
For prostate cancer and gastrointestinal cancer at all stages of the disease, the CA 242 test will be more expressive and sensitive than CA 19-9. The first stage of oncology is determined when the specificity of CA 242 is 90%, and the sensitivity of the CA 242 test is 41%, and CA 19-9 is 29%.
The tumor marker for rectal and colon cancer CA 242 will show higher sensitivity than other tumor markers. If the specificity of the test is 90%, then the sensitivity indicator for tumor markers is as follows:
- CA 242 - 40%;
- CA19-9 - 23%;
- CA 50 - 23%.
Serial determinations of CA 242 identify possible recurrence of colorectal cancer within 5-7 months. Tumor markers help not only to detect cancer, but also to evaluate the treatment being carried out. The specificity of each protein indicates tumor foci.
Important. They learn about damage to the gastrointestinal tract by deviations from the norm of certain specific markers. Different tumor markers indicate different tumor localizations. This gives grounds to carry out other methods of examination.
To make diagnostic information more reliable, a combination of markers is used. To confirm:
- stomach cancer - CA 242 and CEA are examined;
- pancreatic cancer - CA 19-9 and SF 242;
- testicular oncology - hCG and ACE.
If ACE, CEA and CA 19-9 levels are elevated, this indicates metastasis to the liver.
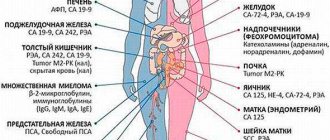
The table shows the main and additional tumor markers for diagnosing cancer of the internal gastrointestinal and genitourinary organs:
| Tumor markers | ||
| Cancer | Basic | Additional |
| stomach | REA, SA 242 | |
| colon: rectum and sigmoid | OEA, SA 19-9, SA 242 | |
| pancreas | SA 19-9, SA-242 | REA, SA-125 |
| gallbladder and ducts | SA 19-9 | AFP |
| liver metastasis | SA 19-9, REA, AFP | |
| hepatocellular carcinoma | AFP | SA 19-9 |
| lung intercellular | NSE | |
| lungs | REA | |
| mammary gland | SA 15-3 | REA |
| chorionepithelioma | hCG | |
| teratoma | AFP, hCG | |
| ovary | CA 125 | |
| uterus | CA 125 | |
| prostate | PSA, St. PSA | |
| testicles | AFP, hCG | NSE |
| Bladder | REA | |
| neuroblastoma | NSE | |
| malignant melanoma | NSE | |
| pheochromocytoma | NSE | |
| carcinoid | NSE | |
We also recommend studying this topic:
What does a blood test for a tumor marker show: explanation of research methods
Types of tumor markers
Among the tumor markers that are effective for diagnosis and treatment monitoring, the following types of studies can be distinguished:
- AFP (alpha feto protein) – some types of liver cancer, ovarian cancer and other types of oncology. AFP may also increase during pregnancy, chronic and acute hepatitis. Blood is taken for analysis.
- Mutations in the B-cell immunoglobulin gene determine B-cell lymphoma. Helps identify characteristic changes in specific B cell genes. Bone marrow, affected tissues, body fluids, and blood are analyzed.
- Mutations in the BCR-ABL1 gene sequence on chromosome 22. Chronic myeloid leukemia, and BCR-ABL-positive acute lymphotic leukemia. Blood and bone marrow are examined.
- Chromogranin A – neuroendocrine tumors (carcinoid tumors and neuroblastomas). It is the most sensitive marker for carcinoid tumors. Blood analysis.
- Gastrin is a hyperplasia of G-cells, tumors that produce this hormone (gastrinoma). Also used in the diagnosis of Zollinger-Ellis syndrome. Blood is examined.
- Beta-hCG – diseases of the testes, ovaries, trophoblasts, germ cell tumors, choriocarcinoma. Increased during pregnancy. Blood and urine analysis.
- Monoclonal immunoglobulins – multiple myeloma and Waldenstorms macroglobulinemia. Cloned plasma cells that overproduce one type of immunoglobulin are commonly used for protein electrophoresis and plasma-free light chain testing. Blood and urine can be tested.
- Redistribution in the structure of T-cell receptor genes - T-cell lymphoma, makes it possible to determine characteristic changes in specific T-cell genes. Bone marrow, tissues, various body fluids, and blood are studied.
CA-125 (Cancer Antigen 125) is effective in detecting and monitoring ovarian cancer. It also increases with other types of malignant cell proliferation, including endometrial cancer, peritonia of the fallopian tubes. Its level may be high in non-cancerous diseases. Among them are endometriosis, inflammatory gynecological diseases of the pelvic cavity, some benign tumors, which include fibroid formations in the uterus and pregnancy. Blood is examined.
Speaking about tumor markers, special mention should be made of the PSA tumor marker, which is very specific and allows one to identify prostate cancer. This indicator is specific, and therefore it can be used for screening with an increased risk of family history, during prostatitis and with increasing age.
CA 242 tumor marker - what does it mean?
The gastrointestinal tumor marker CA 242 refers to a carbohydrate antigen at an increased level in the presence of cancer tumors in the gastrointestinal tract.
Important. In the first stages of cancer, the specificity of CA 242 can reach 90%, the CA 242 test is 41% sensitive. Tumor marker indicators are used to determine the effectiveness of oncology treatment, identify relapses and metastasis.
A specific protein is produced by benign tumor cells and cancer cells. With the appearance of benign diseases, fistulas in the gastrointestinal tract, the tumor marker CA 242 increases slightly. If the tumor is malignant, then the protein becomes more expressive compared to other tumor markers, for example CA 19-9.
Description of tumor markers
When a tumor forms in the body, it transforms the tissues affected by it at the cellular level. Neoplasm tissues differ from healthy ones not only in their structure, but also in their functional parameters. And such tissues, transformed by cancer, often produce special substances that enter the blood, which are called tumor markers. If they are found in a person’s bloodstream, or, for example, in urine excreted, then this most likely indicates the presence of cancer in a person.
Markers help not only determine the presence of cancer, but also show how effective the therapy was. When a tumor is treated during treatment, its tissues die and the tumor disintegrates. The decay process provokes the release of substances formed during this process into the bloodstream, and as a result, the content of tumor markers in the blood increases. But their presence does not necessarily indicate an oncological disease - there are often situations when the level of specific substances increases against the background of ordinary infections or inflammations.
In total, approximately 200 substances produced by various types of tumors are known today. Not all of them have real diagnostic utility - the list of markers used in medicine is much lower.
The analyzes focus specifically on these indicators, which, when detected, will indicate with high accuracy the system or organ affected by the tumor, and this property of tumor markers has found wide application in clinical practice.
What are tumor markers?
A tumor biomarker is a substance (usually a protein molecule) produced either by the cancer cells themselves or by other cells of the body in response to cancer pathology.
Sometimes healthy cells in the body are able to produce such substances in response to certain benign (non-cancerous) conditions. Tumor markers provide information about a tumor, such as how aggressive it is, whether it can be treated with targeted therapy, and how well the tumor responds to treatment.
Tumor markers are proteins or other substances that are produced by cancer cells in higher quantities than normal cells. These biomarkers are found in blood, urine, stool, or other body tissues or fluids.
For some types of neoplasia, the level of a tumor marker reflects the stage (extent) of the disease and/or the patient's prognosis (the likely outcome or course of the disease). An example of this type of tumor marker is α-fetoprotein, which is measured in the blood to assess the stage, prognosis, and track response to treatment of germ cell tumors.
However, increasingly, genomic indicators such as mutated forms of genes, tumor gene expression patterns, or nongenetic changes in the DNA of cancer cells are being used as tumor markers.
Currently, about 60 tumor markers have been characterized in detail and are in clinical use. Some of them are associated with only one type of tumor (specific tumor markers), while others are associated with several types of cancer pathology (nonspecific tumor markers).
This number does not include tumor markers, which are tested using immunophenotyping and immunohistochemistry, which help diagnose cancer and distinguish between tumor types.
At the same time, a “universal” tumor marker that could detect the presence of any type of cancer pathology has not yet been discovered.
Indications for testing
Your doctor may order a test if you have the following symptoms that are similar to stomach cancer:
- frequent vomiting and/or nausea;
- dysfunction of the gastrointestinal tract;
- aversion to foods containing protein;
- unreasonable growth of the abdomen;
- change in the color and consistency of stool (the most dangerous color of stool is black);
- non-cancer symptoms - deteriorating health, low hemoglobin levels that cannot be treated, heredity.
The oncologist will advise you to get tested if you suspect oncology of the female organs, lung or pancreas cancer.
The patient is also recommended to undergo analysis for the level of tumor markers after surgery. After 3-4 weeks, if the tumor is successfully removed, the indicators will decrease. If this does not happen, treatment is continued with other methods - chemotherapy, radiation therapy.
It is recommended to conduct research in case of questionable indications of other tumor markers.
Rules for taking the analysis
For correct diagnosis and treatment monitoring, the patient will have to be tested for the level of the CA 72-4 tumor marker more than once. Many public clinics do not have the necessary equipment to examine and detect markers. To ensure the reliability of the results, it is recommended to take the analysis in the same laboratory. In many cities, research centers for medical tests Invitro, KDL and others have been opened, where you can take any test, including tumor markers for intestinal cancer.
Venous blood is taken to determine the level of cancer antigen CA 72-4. Biological material must be donated in the morning, on an empty stomach. The day before the test, it is undesirable to eat fatty foods. The oncologist who ordered the test must be informed about all medications that the patient is constantly taking or has taken in the last few weeks.
Analysis errors
The tumor marker CA 72-4 is elevated in human serum not only in cases of cancer. Antigen values may be higher than the accepted norm if there are inflammatory processes in the body. This can happen with infectious and bacterial diseases. After treatment, cancer antigen levels return to normal. Increased values are also observed in pregnant women.
Indicators above the accepted norm can also be observed in the following non-oncological diseases:
- stomach ulcer;
- cyst or inflammation of the pancreas;
- bronchopulmonary diseases;
- polyps;
- gastroesophagitis (reflux);
- cirrhosis of the liver;
- Crohn's disease;
- rheumatoid arthritis;
- mastopathy.
Accordingly, normal values of cancer antigen concentration do not guarantee the absence of cancer.
We must not forget that analysis is not the final diagnosis. To accurately diagnose the disease, other research methods are necessary (gastroscopy, MRI, CT, ultrasound, biopsy). The results of tumor marker analysis should not be used as self-diagnosis. Only an oncologist will determine the accuracy of the diagnosis and suggest treatment tactics.
Analysis
For analysis, blood is taken from a vein, and stool analysis is also possible. The analysis is carried out in a laboratory equipped for immunological studies. Mostly they are located at oncology centers. Private laboratories also determine cancer markers, but some tests may not be performed there. In order not to waste time, it is better to first find out what tumor markers are determined there.
Before the study you need to prepare:
- 5 days before the study, the doctor stops taking cytostatics and other drugs that affect the results. If he said that medications must be taken, then this factor will be taken into account when deciphering the results.
- Do not drink alcohol, give up cigarettes (at least for 3 days). Alcohol and nicotine significantly increase the concentration of some tumor markers in the blood.
- The day before the analysis, exclude physical activity.
- Blood from a vein is donated on an empty stomach. You cannot eat for 12 hours, and drink tea, coffee, or other drinks for 6 hours before blood sampling.
- Before donating blood for analysis, you need to sit in front of the office for 10–15 minutes to calm down.
Be sure to read:
Preparation and performance of computed tomography (CT) of the intestine
Before submitting stool for determination of Tu M2-RK, you must not:
- undergo X-ray and endoscopic examination;
- use laxatives;
- give enemas.
Feces are collected in a sterile container.
To correctly diagnose and evaluate the effectiveness of treatment, it is not enough just to detect the presence of tumor markers in the blood. The data obtained must be interpreted correctly.
Indications for the use of tumor marker diagnostics
This type of blood test is prescribed when:
- the doctor suspects cancer in the patient;
- the specialist wants to determine how effective the previous therapy was and track the success of the treatment over time.
Patients who complain of poor appetite, general decreased health, and poor digestion are usually prescribed this test. Another signal of checking the blood for tumor markers is the lack of effectiveness of therapy with vitamins and a diet with a high iron content, against the background of which the patient’s hemoglobin level does not increase.
The gastroscopy technique is widely used in diagnosing cancer, and additional tests are not required so often, since gastroscopic examination provides a fairly complete picture of the disease. But the level of markers in the blood shows well what stage the disease is at. The higher the content of these substances, the more advanced the cancer is, and the more severe the patient’s condition, and it is also much more difficult to treat a patient with a high level of markers. These indicators can be called signals of what the treatment outcome will be: the lower the level of window markers, the greater the patient’s chances of survival.
When a patient has been operated on as part of treatment for stomach cancer, he is tested twice a year for CA 72-4. This is done because any cancerous tumor can relapse at one point. When the tumor is removed, the kidneys remove the resulting residual decay products, and the concentration of foreign glycoproteins in the body gradually decreases, becoming normal after about a year. If the tumor has metastasized, then they remain in a latent state for some time, without showing anything. And only a blood test for tumor markers can reveal a hidden pathological process and detect metastases even before they clearly show their symptoms. The tumor marker CA 72-4 is also useful in cases with relapses of the disease: it is sensitive to them too.
But it should be remembered that the growth of CA 72-4 is not always bad. If the patient has undergone chemotherapy, then a high concentration of this glycoprotein is a good sign of the success of treatment.
Interaction with other markers
A blood test for the tumor marker CA 72-2 has low sensitivity and in most cases the indicators increase in the later stages of cancer. Therefore, when diagnosing oncology, studies of other cancer markers are also required.
What cancer antigens does the CA 72-4 tumor marker interact with?
- CA 242 - is determined mainly in malignant neoplasms. It is synthesized in the mucous epithelium lining the stomach, intestines, and pancreas.
- CA 19-9 - allows you to diagnose malignant processes in the pancreas. Helps predict relapse and assess the effectiveness of surgical treatment and chemotherapy.
- HE4 – rapidly increases in malignant formations of the genital organs in women.
- SCC – indicates the presence of squamous cell carcinoma of any location.
- CA 15-3 - prescribed together with other markers for the diagnosis, monitoring and prevention of relapse of breast carcinoma.
- CA 125 – necessary for diagnosing ovarian cancer. It increases with severe benign inflammation in the pelvis, abdomen and chest.
- AFP - indicators increase with neoplasms in the mammary gland, liver and gastrointestinal tract.
- CA 50 - indicates liver cancer and chronic inflammation of the pancreas.
- MSA is an auxiliary analysis that is prescribed for the comprehensive diagnosis of cancer formations in the gastrointestinal tract.
- CEA (CEA) – used in conjunction with most tumor markers for suspected breast, ovarian, intestinal, stomach and pancreatic cancer. It increases rapidly if the tumor metastasizes.
A combined study of cancer antigens and instrumental examinations makes it possible to make a diagnosis with high accuracy, detect metastases at an early stage and determine the likelihood of relapse.
The importance of further diagnosis
If the interpretation of the results on CA 72 4 showed negative elevated values, it is imperative to undergo other tests that confirmed or refuted the diagnosis of cancer. This can be a biopsy, X-ray, MRI, CT, as well as studies of other tumor markers that increase in response to the development of a particular type of cancer.
Recently, there has been a significant expansion of the concept of what can be used as a tumor marker. New tests have been invented that study changes in genetic material (DNA, RNA) more often than the proteins themselves.
Changes in gene structure are usually detected in certain types of malignant tumors, which can be used as tumor markers for prognosis, treatment guidance and early diagnosis. In addition, the development of technology has led to the creation of tests that are capable of comprehensively assessing several genetic tumor markers in a panel simultaneously. In this case, much more accurate and detailed information about neoplasms is obtained.
Interpretation of results
Important! Standards vary depending on the reagents and equipment used in each particular laboratory.
Therefore, when interpreting the results, it is necessary to use the standards adopted in the laboratory where the analysis was carried out. You also need to pay attention to the units of measurement. To avoid errors when interpreting results over time, it is necessary to do the analysis in the same laboratory, since different institutions use different methods and reagents. In addition, conducting only one test for CA 72-4 and making an accurate diagnosis only on its basis is categorically unacceptable. It is required to conduct a comprehensive, comprehensive examination using additional diagnostic tests, including instrumental ones.
Reference values:
- 0-6.9 U/ml (Helix and Invitro laboratories);
- 0-4.6 IU/ml (handbook of laboratory diagnostics edited by MD, Prof. Kishkun)
Decoding the results. Tumor marker CA 72-4 normal
Normal tumor marker values range from 0 to 6.9 units/ml.
During the initial diagnosis, obtaining such a result does not completely exclude cancer. The fact is that the release of glycoprotein increases with tumor growth, so at the initial stage of the process the analysis may be normal. The highest sensitivity of the tumor marker is demonstrated for gastric cancer. It is 80% in the early stages and increases as the lesion grows. It is recommended to repeat the analysis even in the case of a slight deviation from the norm and borderline results.
When normal glycoprotein values are obtained after a tumor has been identified and treated, conclusions can be drawn about the effectiveness of treatment
It is important to remember that the decrease in marker concentration occurs gradually during chemotherapy. And even with surgical treatment, you shouldn’t count on a sharp decrease in the first weeks.
For reference. If CA 72-4 is normal when monitored for several years following successful treatment, then we can say that there is no relapse.
CA 72-4 elevated - reasons
An increase in CA 72-4 is assessed differently depending on whether it is prescribed for the first time when an oncological process is suspected or is used to monitor identified oncology.
A slight increase in the marker may be a sign of both the initial stages of a malignant neoplasm and benign processes.
An increase in malignant processes is observed with damage to:
- stomach;
- breasts;
- Tumor metastasis;
- Intestines (mainly colorectal cancer);
- Ovarian cancer;
- Pancreas;
- Lungs;
- Uterus.
In this case, the greatest sensitivity is observed in relation to the stomach. Lesions of the lungs are less likely than other organs to manifest themselves in laboratory tests with an increase in CA 72-4.
Somatic diseases that can lead to deviations from the norm CA 72-4:
- Autoimmune diseases;
- Mastopathy;
- Pancreatitis;
- Ovarian cysts;
- Chronic lung diseases;
- Inflammation of various parts of the gastrointestinal tract;
- Chronic liver diseases (cirrhosis, hepatitis).
In addition, the doctor always clarifies about the possibility of pregnancy at the time of taking blood for analysis, since this circumstance also contributes to an increase in tumor marker numbers.
CA 72-4 for oncology
If an oncological process is detected after successful treatment, it is recommended to take CA 72-4 to monitor a possible relapse.
Sensitivity is higher for stomach cancer, but for colorectal cancer it is only about 40 percent. An increase in the level of the marker in the long-term period indicates a possible relapse of the process and requires further examination with instrumental and additional laboratory methods. The decrease in tumor marker levels during treatment occurs gradually.
For reference. After an oncological disease has been identified and surgical treatment has been carried out, it is recommended to take the test no earlier than a month later, since until this moment the pre-operative level is observed. An increase in the CA 72-4 marker after treatment may indicate its ineffectiveness.
A test for the CA 72-4 marker is usually prescribed in parallel with other tumor markers and biochemical laboratory parameters, depending on the suspected process. This increases the diagnostic value of the study and provides more information to the oncologist.
If elevated or close to normal values are detected, a repeat study is always recommended to confirm the results. The doctor compares the anamnesis (disease history), symptoms, and examination data to prescribe an analysis.
Diagnosis is never based on data from a single analysis. The oncologist always resorts to additional methods in the form of instrumental research and biochemical parameters. Concomitant conditions are taken into account. For example, pregnancy or benign breast disease may result in elevated CA 72-4 test results.
For reference. Monitoring glycoprotein levels after treatment of an oncological process is mandatory. It is very sensitive to relapses, therefore it is recommended for regular monitoring in people with stomach cancer and other oncological processes if there is an increase during the detection of the disease.
Decoding
After conducting a study of the CA 72-4 tumor marker, decoding involves an accurate determination of the antigen concentration in the blood. If after treatment of oncology the level of tumor marker in the blood still exceeds 6.9 U/ml, such therapy can be considered ineffective. If an average level of antigen is detected in the blood, we can talk about the possible presence of the following pathologies:
- Disorders of the liver, for example, during cirrhosis;
- Cysts of the gastrointestinal tract, ovaries, and uterus;
- Diseases of the reproductive system in women;
- Breast cysts;
- Blood diseases;
- Certain rheumatic problems.
Tumor markers are deciphered within two days after the analysis. In some cases, a decrease in the level of the CA 72-4 marker is observed. This indicates the absence of malignant neoplasms in the body, or that they are at the initial stage of development, when the production of this antigen is not yet stimulated. Based on what tests were obtained during the study of the CA 72-4 tumor marker, additional examinations may be prescribed.
What does the tumor marker CA 72-4 show when deciphering a blood test?
Decoding the tumor marker CA 7204 is used in the diagnosis of stomach cancer and mucinous cancer (adenocarcinoma) of the ovaries (used in combination with laboratory tests for determining CEA and CA 125).
CA 72-4 is a specific protein with a molecular weight of about 400 kDa, which is a mucinoid tumor-associated glycoprotein circulating in the blood serum, the surface of which contains a number of epitopes.
CA 72-4 has been identified immunohistochemically in tumor tissue from a number of organs, including colon cancer, non-small cell lung cancer, and gastric cancer. It has also been found in various fetal tissues. It is characteristic that CA 72-4 is practically not found in the tissues of an adult organism.
Biological material: Blood serum (plasma).
Research methods: RIA, ELISA using 2 monoclonal antibodies (CC 49 to highly purified TAG 72 and labeled antibodies B 72.3 to metastatic breast cancer cells).
Normal and borderline values: In healthy adults, the normal value of the tumor marker CA 72-4 when deciphered is 2.5-4.0 ng/ml. The cut-off values for deciphering CA 72-4 in serum/plasma analysis are 6.7 ng/ml, or 3.8 U/ml.
Reasons for increasing cancer antigen
The main malignant processes in the human body, in which the CA 724 tumor marker produces increased values:
- Oncological pathologies of the gastrointestinal tract:
- Colon cancer;
- Gastric adenocarcinoma;
- Malignant tumor of the esophagus;
- Tumor in the pancreas.
- Ovarian adenocarcinoma in women and testicular epithelial tumor in men;
- Small and large cell lung cancer;
- Adenocarcinoma of the mammary glands;
- Metastases in the liver.
Tumor marker CA 72-4
Tumor marker CA 72-4 is a complex mucin-type glycoprotein. Like other tumor markers, it is found in the adult body in extremely low concentrations. This glycoprotein is synthesized in large quantities in fetal tissues. CA 72-4 is actively produced by cells of various malignant tumors, as well as in some other non-oncological pathological conditions.
In clinical practice, the CA 72-4 tumor marker is widely used for:
- diagnostics of oncological diseases of the stomach;
- monitoring the dynamics of tumor processes and the formation of metastases;
- control over the therapy of oncological and non-oncological pathologies of various origins;
- diagnosing malignant and benign ovarian tumors.
What is CA2+?
Simultaneously with the analysis for the tumor marker CA 72-4, not only blood is given for cancer markers, but also other laboratory tests, instrumental diagnostics are carried out, and in some cases, detection of Ca2+ in blood serum and saliva is prescribed.
Ca2+ is free ionized calcium that plays an important role in many body processes. Hypercalcemia occurs when the bond between calcium ions and albumin is disrupted by acidosis, which can occur in any stage of cancer. If tumor marker 72-4 and calcium are elevated, then in half of the cases this indicates the presence of malignant, progressive neoplasms.
Indications for analysis
Blood donation for tumor markers is carried out for two possible reasons: either there is a suspicion of cancer, or against the background of treatment, in order to track the dynamics of tumor decay.
Most often, patients receive the prescription due to complaints of poor health, lack of appetite or dyspeptic disorders. Reduced hemoglobin and the ineffectiveness of vitamin therapy and an iron-containing diet also signal the doctor about the need to look at the level of tumor markers.
After gastroscopy, this analysis is extremely rarely needed, since the clinical picture is usually clear. However, the level of these substances in the blood serves as a very reliable reflection of the advanced state of the disease. The higher the level of specific tumor markers, the more severe the patient’s condition and the more difficult his treatment. We can say that the level of tumor markers determines the expected outcome for a particular patient, indicating the likely outcome of treatment, the chances of survival of the patient or the need for surgery.
After surgery for gastric cancer, tumor markers must be reviewed a couple of times a year, since any oncological pathology tends to recur. After tumor removal, the kidneys eliminate all decay products, and the level of foreign tumor glycoproteins gradually decreases, reaching normal values the very next year. When a tumor metastasizes, there is a latent period when the metastases do not manifest themselves in any way. Analysis for tumor markers allows one to suspect metastases to other organs long before their clinical manifestation. The analysis for the cancer tumor marker CA 72-4 remains sensitive even during relapses.
However, an increase in the CA 72-4 tumor marker will not always be a bad sign. High levels of this glycoprotein in the blood are a good prognostic sign after chemotherapy.
What to do if tumor markers are detected?
An increased concentration of tumor markers is in no way a criterion for diagnosing cancer. These substances may appear in greater quantities in the blood during benign diseases. In addition, determining the concentration of tumor markers over time has the greatest diagnostic value: has their number decreased or increased after surgery or conservative therapy. Such screening studies are carried out monthly, if metastases are suspected, to monitor the growth of a tumor that cannot be removed for one reason or another.
Be sure to read:
Histological examination of intestinal tissue: preparation and implementation
To diagnose intestinal cancer, especially in the early stages, analysis of tumor markers is not enough. If only because these substances enter the bloodstream during intensive tumor growth.
A doctor will suspect bowel cancer when a patient comes to him with the following alarming symptoms:
- sudden weight loss;
- abdominal pain;
- dyspeptic disorders.
To identify malignant intestinal tumors, the following is carried out:
- digital examination of the rectum;
- sigmoidoscopy;
- irrigoscopy;
- MRI, , ultrasound;
- radionuclide studies;
- endoscopy with biopsy.
The most accurate data is obtained by performing a biopsy and subsequent study of tissues and cells - histological examination. It allows you to determine the stage of cancer and therapeutic strategy.
The results exceed the norm. Should we panic?
So, what to expect if the stomach tumor marker is elevated? If a person is at risk and is told that the level of the marker CA 72-4 or CA 19-9 is too high, you should not immediately consider yourself sick. Data obtained after one or two analyzes are not enough.
In addition to identifying markers, a lot of research still needs to be done. Additional tests either confirm or refute the hypothesis of cancer. The stomach tumor marker itself can give a false positive result.
Once suspicions of cancer arise, you need to undergo an MRI, ultrasound and gastroscopy. Without gastroscopy, no diagnosis can be considered correct.
What tumor marker indicates bowel cancer?
There is not yet a specific tumor marker that can be used to speak with a reasonable degree of confidence about the presence of a malignant tumor in the intestine. However, a comprehensive analysis with the determination of several different biomarkers can form a reasonable suspicion and become the basis for a serious diagnostic study.
Markers determined by blood tests
Carcinoembryonic antigen (CEA) level is the tumor marker most commonly used in colorectal cancer. Its level can be checked preoperatively for prognosis, used during therapy to assess response to treatment, or after completion of therapy to monitor relapse.
CA 19-9 is a non-tumor blood marker that may be elevated in colorectal cancer.
Chromosome 18q loss of heterozygosity (18qLOH) is a tissue marker often used in patients with stage II or III colorectal cancer. May affect prognosis.
Tumor tissue markers (analysis of stool and biopsy material)
MSI (microsatellite instability) is a way to measure mismatch repair (MMR) deficiency in tumor DNA. MMR deficiency leads to increased mutations in colon cells, which contributes in part to the development of colon cancer.
- MSI can be used to identify early-stage colon cancer that may require more aggressive treatment or to identify patients who should undergo further genetic testing due to the risk of a familial syndrome associated with multiple types of cancer.
- MSI identifies tumors as MSI-high (MSI-H) or MSI-stable and MSI-low.
K-RAS mutations - Specific mutations in the K-RAS gene can predict whether a patient may benefit from treatment with multiple biological treatments.
BRAF mutations - usually associated with the V600E mutation. May be a predictor of prognosis after diagnosis of colorectal cancer.
Purpose of the study
Stomach cancer ranks fourth in the structure of all malignant diseases. According to medical statistics, it is more common in men (35.4%) than in women (25.8%) among all cancer pathologies. The incidence rate increases every year. Stomach cancer mainly occurs in the age group after 50 years, but recently the age of patients has decreased.
The most effective treatment, while maintaining ability to work and quality of life, is possible only in the early stages of the disease. Stomach cancer is asymptomatic in the initial stages. The patient does not show any complaints at this time. Severe clinical symptoms can appear only when the tumor is large, when treatment is already ineffective.
Blood test for tumor markers
The main purposes of prescribing tests for stomach tumor markers are:
- Early diagnosis of malignant neoplasms in individuals with a hereditary predisposition. Even with negative results, such patients need to undergo such tests once every 6-12 months.
- Detection of a low-quality tumor in patients with characteristic complaints.
- Making a diagnosis of stomach cancer.
- Determination of the prognosis, nosological form of the pathological formation, selection of the necessary treatment method. If a patient has cancer of another location, detection of a large number of specific proteins in the blood contributes to the early detection of metastases in the stomach.
- For dynamic monitoring of the patient's condition after surgery or chemotherapy.
A decrease in the level of tumor markers indicates the effectiveness of antitumor treatment. If these indicators increase, therapy correction is necessary (additional courses of chemotherapy, increasing the dose or time of irradiation).
If the patient has no complaints and general objective signs of cancer, then such an analysis is not performed as a screening test.
Nonspecific markers
Nonspecific markers are determined in various malignant tumors, and often in non-cancerous pathologies.
In colorectal cancer, several nonspecific tumor markers are more often used. Determining each of them has its own task - testing for sensitivity to a specific therapy, diagnosing relapses, monitoring the effectiveness of treatment
Examples of markers used in colorectal cancer.
Mutation of the DPD gene in the blood. Types of neoplasms: stomach, pancreatic, breast and colorectal cancer. Used to predict the risk of toxic reactions to 5-fluorouracil therapy.
BRAF V600 mutations in tumors. Types of neoplasms: cutaneous melanoma, Erdheim-Chester disease, colorectal cancer and non-small cell lung cancer. Used to select patients who are most likely to benefit from treatment with specific targeted therapies.
Mutation of the KRAS gene - in the tumor. Types of neoplasms: colorectal cancer and non-small cell lung cancer. Used to determine whether a particular type of targeted therapy is appropriate for treatment.
When and how are tests taken?
All tests for stomach tumor markers are taken in the morning, on an empty stomach. There are also dietary restrictions the day before the test.
What are the requirements for the obtained result to be as reliable as possible?
- Do not eat 12 hours before the test.
- If you are taking the vitamin biotin, you must stop taking it 8 hours in advance.
- 48 hours before donating blood, do not eat anything fried, fatty or spicy. Only boiled, steamed food that does not cause irritation to the mucous membranes.
- You should also not smoke, drink coffee, tea or even mineral water. It is permissible to drink only clean water.
Smoking patients are warned that cigarettes are also prohibited several hours before the procedure. Smoking may also affect the results. By the way, tobacco smoke contributes to the development of stomach cancer. Since carcinogens enter the organ directly with it. And besides, nicotine enhances the production of hydrochloric acid.
First screening. What tests are taken?
Screenings are carried out to determine risk groups. These types of tests are not diagnostic. However, they are necessary to understand whether further research is needed and whether a person should spend money and time on other tests, analyzes and complex studies.
Primary tumor markers are proteins whose enzymes are waste products of the tumor. They are determined first, as they have greater sensitivity. They use CA 15-3, CEA, CA-50 and an additional analysis - a marker for pancreatic carcinoma CA 242. The gastric tumor marker CA 72-4 is most informative for making a diagnosis.
How were tumor markers discovered?
For the first time, scientists such as Lev Zilber and Harry Izrailevich Abelev discovered that alpha protein may indicate liver cancer. They accidentally discovered these substances while studying the composition of tumor hepatocytes (liver cells).
Alpha protein is a protein that is produced by the placenta. The researchers had absolutely no idea that they would find it in these cells. They were looking for a virus and found the first liver tumor marker.
How often do you get your blood tested?
If a person has already had some type of cancer, he needs to be monitored more often so as not to miss the resumption of tumor growth. It is recommended that such people donate blood once every 6 months for one specific marker. Just to find out if there is a relapse. However, when there was no tumor, but the person is at risk, he should also be checked every few years. You cannot skip the development of the first stage. This is the best time for treatment.
For completely healthy people who are not at risk, there is no need to donate blood for stomach tumor markers. But for your own peace of mind, you can take one test at the nearest private clinic, without a referral.