The well-known epidemic has forced us to take our health more seriously. Recently, a long-known examination technology, computed tomography, or CT, has become the crowning one.
Today, hardly anyone with a mild cough or chest pain considers it necessary to undergo this procedure. For the first time in history, queues are forming in front of CT rooms, machines are working almost around the clock, and people are trying to get examined, often bypassing the doctor’s decision.
Is everything so smooth? Is it possible to prescribe a CT scan for yourself? Is there any harm and is CT capable of seeing everything that its new fans want to diagnose?
We understand the nuances of the technology in detail and answer all questions.
How did X-rays become CT scans?
Traditional radiography is carried out with a source and a photographic plate even today.
Modern computed tomography, like the familiar radiography (“X-ray”), is one of many types of studying objects from the inside using radiation of the same name, which got its name thanks to its discoverer, Wilhelm Roentgen.
He found out that a number of materials are capable of emitting radiation without external influences, leaving images on photographic plates, which at that time replaced the photographic film we were accustomed to.
A detailed study of X-rays revealed that the effect is based on processes associated with the movement of electrons from the source of the rays, which are in many ways similar to gamma radiation.
"Analog" X-ray
Including the strength of permeability: like gamma, X-ray radiation passes through almost any material without reflection or refraction (exactly directly), and is also ionizing (can cause radiation sickness).
However, X-rays are absorbed, and different substances do so at different rates. It shines through soft tissues, partly solid organic materials, and is almost completely retained in metals.
Scheme of operation of modern X-ray machines
Thanks to the “translucency” and the effect of fluorescence (glow) of materials under the influence of x-rays, fluoroscopy (observation of an image on a fluorescent screen) and x-ray photography (radiography) appeared, which became popular methods of medical and industrial radiographic methods of non-destructive research.
In 1917, Radon invented an algorithm that made it possible to create a three-dimensional model of the body under study from sequentially taken x-rays with varying radiation strength.
A CT scan is very similar to an X-ray
In 1963, a full-fledged mathematical model for practical recalculation appeared, and in 1969, the first apparatus for tomographic research appeared, for which 3 years later the creators received the Nobel Prize.
IT HAPPENS: the first tomograph was created by EMI with money received from sales of Beatles records that were recorded in its studios.
Relaxation of the diaphragm
Relaxation of the diaphragm
- this is total or limited relaxation and high standing of the dome of the thoraco-abdominal septum with prolapse of the adjacent abdominal organs into the chest. Clinically manifested by cardiovascular, respiratory, and dyspeptic disorders.
The predominance of certain symptoms depends on the location and severity of the pathological process. The leading diagnostic methods are x-ray examination and computed tomography of the chest organs.
The only treatment option is auto- or alloplasty of the diaphragmatic dome or part of it.
Relaxation of the diaphragm (paralysis of the diaphragm, megaphrenia, primary diaphragm) is caused by sudden dystrophic changes in the muscular part of the organ or a violation of its innervation. It can be congenital or acquired. Complete (total) relaxation of the thoraco-abdominal septum is more common on the left.
A limited protrusion of its area (diaphragmatic diverticulum) is usually localized in the anterior medial part of the right dome. In children, relaxation of the diaphragm occurs very rarely; disorders develop gradually as a person grows and under the influence of external factors. The first symptoms appear at 25-30 years of age.
Men engaged in heavy physical labor suffer more often.
Relaxation of the diaphragm
The high standing of the diaphragmatic dome is caused by pronounced thinning, up to complete absence, of its muscle layer.
This structure of the abdominal barrier is often caused by impaired development of the organ in the prenatal period. Another common cause is paralysis of the diaphragmatic muscles.
The following groups of etiological factors leading to relaxation of the diaphragm vault are distinguished:
- Embryogenesis disorders.
These include defects in the formation of myotomes and further differentiation of muscle elements, underdevelopment or intrauterine damage to the phrenic nerve. Congenital relaxation of the diaphragm is often combined with other malformations of internal organs. - Damage to the diaphragmatic muscle.
It can be inflammatory and traumatic. There is independent inflammation (diaphragmatitis) and secondary damage to the diaphragm. The latter appears when the pathological process spreads from adjacent organs, for example, with subdiaphragmatic abscesses, pleural empyema. - Paralysis of the diaphragmatic dome.
Occurs with various types of disorders of the innervation of the diaphragm. Traumatic processes, including surgical interventions, lead to nerve damage. Total paralysis is caused by severe systemic neurological diseases (poliomyelitis, syringomyelia). Local lesions occur as a result of tumor invasion of the nerve trunk.
With a congenital anomaly leading to relaxation of the thoraco-abdominal septum, an almost complete absence of muscle tissue is detected. The thin diaphragm consists of pleural and peritoneal layers.
With acquired pathology, muscle dystrophy of varying degrees of severity is observed. Lack of muscle tone leads to the loss of part of the functional abilities of the diaphragmatic vault.
Due to the difference in pressure in the chest and abdominal cavities, the internal organs stretch the diaphragm, contributing to its full or partial protrusion into the chest area.
The pathological process is accompanied by compression of the lung and the development of atelectasis on the affected side, and displacement of the mediastinum in the opposite direction. Relaxation of the left dome lifts the abdominal organs upward. Volvulus of the stomach and splenic flexure of the colon occurs.
Kinks appear in the esophagus, blood vessels of the pancreas and spleen, leading to transient ischemia of the organs. Due to impaired venous outflow, the veins of the esophagus dilate and bleeding occurs. Relaxation of the right dome (usually partial) causes local deformation of the liver.
Pathological changes in internal organs and disorders of their functions depend on the causes, prevalence and localization of protrusion of the diaphragmatic septum.
According to the time of occurrence and etiological factors, relaxation of the diaphragm is divided into congenital and acquired. The process can be located on the right or left, and can be total or partial.
Depending on the clinical course, there are 4 options for relaxation of the diaphragmatic vault:
- Asymptomatic
. There are no manifestations of the disease. Relaxation is detected incidentally on chest x-ray. - With erased clinical symptoms
. This form is characteristic of a limited, often right-sided process. The patient usually does not attach importance to the unstable, mild symptoms of the disease. - With a detailed clinical picture
. It manifests itself in a variety of symptoms, depending on the degree of damage to the respiratory, digestive, and cardiovascular systems. - Complicated
. It is characterized by the development of serious complications (volvulus, stomach and intestinal ulcers, gastrointestinal bleeding, etc.).
Clinical manifestations of relaxation of the diaphragmatic dome are varied. Symptoms are more pronounced with congenital pathology. Limited relaxation of the diaphragm area can occur latently or with minimal complaints.
In the total absence of tone of the thoraco-abdominal septum, the disease is accompanied by respiratory, cardiovascular, and dyspeptic syndromes.
Most patients present general complaints of episodes of weakness and unmotivated weight loss.
Respiratory disorders are manifested by attacks of shortness of breath and dry, unproductive, painful cough with little physical activity, change in body position, or after eating.
A clear connection between symptoms and food intake is a pathognomonic sign of diseases of the diaphragmatic dome. Cardiac activity suffers. Tachycardia, cardiac arrhythmias, and palpitations occur.
Periodically, the patient is bothered by chest pain of a pressing, squeezing nature, reminiscent of cardialgia during angina pectoris.
The leading signs of diaphragm pathology are digestive disorders. Attacks of acute pain in the epigastric region, right or left hypochondrium also occur after eating. The pain is quite intense, lasting from 20-30 minutes to 2-3 hours, then it stops on its own.
When the esophagus is bent, swallowing is impaired. In some cases, the patient is able to swallow large pieces of solid food, but chokes on liquid (paradoxical dysphagia). Patients often complain of heartburn, hiccups, belching, nausea, and less commonly, vomiting.
Patients are concerned about flatulence and periodic constipation.
Under the influence of a number of factors that increase intra-abdominal pressure, relaxation of the diaphragm, especially congenital, gradually progresses. The dome of the thoraco-abdominal obstruction can reach the level of the second rib. In this case, a pronounced displacement of internal organs occurs. The lung contracts, and areas of atelectasis form.
When the stomach and intestines are pulled up, they occupy the wrong position. Because of this, severe complications from the digestive system develop. The most common of them are volvulus of the stomach, intestines, ulcerative processes, and bleeding.
Leading specialists in the field of surgery describe isolated cases of gastric gangrene.
If relaxation of the diaphragmatic dome is suspected, a surgeon will conduct a diagnostic search. When interviewing the patient, he clarifies the history of injuries and operations in the chest and abdomen, inflammatory processes in the lungs, pleura, mediastinum, and upper abdominal cavity. To confirm the diagnosis, the following studies are performed:
- Inspection
. Sometimes it is visually possible to determine the paradoxical movement of one of the diaphragmatic domes. The diaphragm rises during inhalation and falls during exhalation. There is a positive Hoover's sign - elevation of one of the costal arches and outward displacement during deep inspiration. - Percussion
. The upward expansion of Traube's subphrenic space is determined. The lower border of the lung is located at the level of the II-IV rib along the anterior surface of the chest wall. The boundaries of absolute and relative cardiac dullness shift in the opposite direction. - Auscultation
. Decreased breathing is heard in the basal parts of the lungs. Auscultation of the heart reveals muffled sounds, increased heart rate, and rhythm disturbances. In the lower part of the chest in front you can hear intestinal peristalsis and splashing sounds. - Functional Research
. Spirometry makes it possible to identify restrictive disorders of external respiration function, a significant decrease in the vital capacity of the lungs. The ECG reveals slowing of intraventricular conduction, extrasystole, and signs of myocardial ischemia. - Radiation diagnostics.
X-ray and CT scan of the chest are the most informative methods for studying the diaphragm. The radiograph visualizes the high location of one of the domes (level II–V ribs). Fluoroscopy reveals paradoxical movement of the diaphragmatic vault. The use of contrast makes it possible to identify kinks in the esophagus, stomach, and upward displacement of the digestive organs. CT most accurately determines the degree of relaxation and helps to recognize secondary pathology of internal organs.
CT scan of the chest. Relaxation, high position of the right dome of the diaphragm
Complete relaxation of the abdominal obstruction should be differentiated from its rupture and diaphragmatic hernias. Sometimes the high standing of one of the vaults can hide a basal spontaneous pneumothorax. Partial relaxation often masks neoplastic and inflammatory processes of internal organs, pleura and peritoneum, liver and pericardial cysts.
The only treatment for complete or partial relaxation is surgical. Patients with a latent form of the disease and an erased clinical picture are subject to dynamic observation.
They are advised to avoid excessive physical activity, eat small portions often, and avoid overeating. If the process progresses or there are severe cardiovascular, respiratory or dyspeptic disorders, surgical intervention is indicated.
Relaxation of the diaphragm, complicated by organ rupture, volvulus of the stomach, intestines, or bleeding, is subject to emergency surgical correction.
Taking into account the localization of the pathological process, laparotomy or thoracotomy is performed. A minimally invasive thoracoscopic approach has been developed.
With moderate relaxation with partial preservation of muscle tone, phrenoplication is possible - excision of a thinned part of an organ with its subsequent doubling or tripling with its own diaphragmatic tissues.
Complete relaxation of the right or left dome is an indication for plastic surgery with synthetic material (Teflon, polyvinyl alcohol, terylene). In pediatric surgery, the abdominal barrier is sutured with parallel rows of corrugated sutures, which are then tightened, form folds and lower the diaphragm.
Timely diagnosis and correct surgical tactics lead to complete recovery. The prognosis is worsened by life-threatening complications and severe concomitant pathology. Prenatal ultrasound can reveal the absence of diaphragmatic muscles in the fetus.
Detected relaxation must be corrected before complications develop.
Prevention of injuries, diagnosis and adequate treatment of inflammatory processes of the pulmonary parenchyma, pleura, mediastinum, drainage of subdiaphragmatic abscesses help to avoid acquired paralysis of the diaphragm.
Source: https://www.KrasotaiMedicina.ru/diseases/zabolevanija_pulmonology/diaphragmatic-relaxation
X-ray and tomography. What are the differences?
Examination using tomography is very different from x-ray
Computed tomography is a type of examination using X-rays that can give a three-dimensional layer-by-layer picture of an object, as they say, from the inside.
A classic X-ray machine , which is used to take familiar black-and-white photographs of broken bones or fluorography of the lungs, uses a rigidly installed source of X-ray radiation.
With it, he illuminates the object once, but in many beams. Each one leaves traces on the sensitive substrate behind the body under study, differing in their intensity.
The more the area under study absorbs rays, the dimmer the image. This is why x-rays show well the solid components of the body (bones, tumors, foreign bodies) - their absorption due to their composition is higher than that of soft tissues.
Modern X-ray uses a digital detector, but cannot “drive around” and shoot 3D
Today there are digital X-ray machines in which the usual “image”—a substrate sensitive to X-ray radiation—is replaced by a digital detector that allows images to be taken “dynamically,” that is, in real time.
However, the principle of operation remains the same: the image is taken instantly over the entire area under study, giving a flat one-dimensional image “through and through”.
Unlike the X-ray procedure, CT uses the method of layer-by-layer “transillumination” of the object under study with discretely (certain levels) increasing power of the X-ray beam, which is recorded on a digital detector.
The familiar “dental X-ray” has long been replaced by tomography
With each step, increasing the intensity of the radiation, the device “climbs” deeper - the X-ray radiation step by step takes pictures of the object to a thickness of 1-3 centimeters. The result is then put together.
The study produces many images that, one after another, show the entire volume of the body being examined. Then they are combined according to special algorithms using a computer into a single three-dimensional digital model, allowing you to “twist” the object under study, examining it from the inside from all sides.
Benefits of CT
Tomography allows you to build complex three-dimensional models
If an anomaly on an X-ray can hide behind something else that absorbs X-ray radiation better (this is how many tumors “disappear” behind bones), it cannot escape from a CT scan: a specialist can turn the image to the desired side.
In the same way, using three-dimensional images, the condition of complex surfaces that are practically undetectable on x-rays is assessed. For example, not only the size, but also the shape of organs from all sides.
What’s even more interesting is that with the help of modern CT devices with a high generation rate of radiation beams, it is possible to obtain images in dynamics. See not only what, but also how.
There is no other way to see the circulatory system in dynamics.
Therefore, the results of a CT examination are much closer to ultrasonic examination methods (ultrasound) than to conventional x-rays, from which they inherited only the basic principle of operation.
However, CT is seriously different from ultrasound. The deciphering of pictures obtained using ultrasound rests entirely with the specialist conducting a specific study. Already at the stage of the shooting itself, since the devices require specific settings for the patient and the area being examined.
An international standard has been developed for the use of CT in medicine , to which all existing medical complexes comply. Therefore, CT is completely objective, like X-rays - at least until the stage of obtaining the image.
Who has the right to do x-rays in a dental clinic?
Dentists have always had many questions on this topic. Let's take a closer look and answer the most important of them.
Question No. 1: Which personnel are legally entitled to conduct x-ray examinations?
According to the current legislation of the Russian Federation, only two types of medical specialties have the right to conduct X-ray examinations in medicine:
- Radiologist
- X-ray technician
Question No. 2: Does a dentist have the right to conduct X-ray examinations himself?
A dentist of any specialization DOES NOT HAVE THE RIGHT to conduct X-ray examinations. At all. No way. It’s stupid, unreasonable, offensive – but it’s a fact.
Question No. 3: Can a dentist receive an improvement that gives him the right to independently conduct x-ray examinations?
As we found out, to independently conduct x-ray studies, you need to be either a radiologist or an x-ray technician.
A dentist CANNOT undergo professional retraining (primary specialization, primary) in medical radiology. What is prohibited? Here's what:
There is such a document: ORDER of the Ministry of Health of the Russian Federation dated July 23, 2010 N 541n “ON THE APPROVAL OF A UNIFIED QUALIFICATION DIRECTORY OF POSITIONS OF MANAGERS, SPECIALISTS AND EMPLOYEES, SECTION “QUALIFICATION CHARACTERISTICS OF POSITIONS OF EMPLOYEES IN THE HEALTH FIELD "WOUNDS."
It specifies the qualification requirements for the position of “radiologist”: Higher professional education in one of the specialties: “General Medicine”, “Pediatrics”, “Medical Biophysics”, “Medical Cybernetics”, “Dentistry” and postgraduate professional education (internship and (or) residency) in the specialty “Radiology” or professional retraining in the specialty “Radiology” with one of the specialties “Aviation and space medicine”, “Obstetrics and gynecology”, “Anesthesiology-reanimatology”, “Diving medicine”, “Dermatovenereology” ", "Pediatric surgery", "Pediatric oncology", "Pediatric urology-andrology", "Pediatric endocrinology", "Gastroenterology", "Hematology", "Geriatrics", "Infectious diseases", "Cardiology", "Coloproctology", " Nephrology”, “Neurology”, “Neonatology”, “Neurosurgery”, “General medical practice”, “Oncology”, “Otorhinolaryngology”, “Ophthalmology”, “Pediatrics”, “Plastic surgery”, “Occupational pathology”, “Pulmonology”, “Rheumatology”, “X-ray endovascular diagnosis and treatment”, “Cardiovascular surgery”, “Emergency medical care”, “Thoracic surgery”, “Therapy”, “Traumatology and orthopedics”, “Urology”, “Phthisiology”, “Surgery” , “Maxillofacial surgery”, “Endocrinology” without showing work experience.
As you can see, the primary radiology program remains, but there is no dentistry there.
Those. a doctor who graduated from the Faculty of Dentistry, at the moment, CANNOT become a radiologist through primary training.
Unless he can go to a 2-year residency in radiology. And this, in fact, is a complete change of profession and 2 years of full-time study.
The path to radiology through primary care is closed for a dentist.
Question No. 4: Which medical staff can undergo training and become an x-ray technician?
In accordance with the same order of the Ministry of Health of the Russian Federation No. 541n, requirements for the qualifications of an x-ray technician are established. There are only two requirements:
- Secondary vocational education in the specialty “Nursing”, “General Medicine”, “Midwifery”, “Dentistry”, “Preventive Dentistry”, “Orthopedic Dentistry”
- Certificate of a specialist in the specialty “Radiology” without any work experience requirements.
An X-ray technician is a specialist with a SECONDARY medical education. Not with the highest! Professional training in the specialty “X-ray technician” is carried out in medical colleges on the basis of secondary medical education (primary specialization 432 hours, distance learning is possible).
Accordingly, a doctor with a higher medical education CANNOT train as an x-ray technician in accordance with the qualification requirements under Order No. 541n.
Now, regarding professions, who exactly can undergo advanced training and receive the qualification “X-ray technician” in accordance with Order No. 541n?
- “Nursing” is a nurse. This means that all nurses can become x-ray technicians.
- “Medicine” is a paramedic. This means that any paramedic can train to become an x-ray technician.
- “Midwifery” is an obstetrician(s). Accordingly, any midwife (not to be confused with the specialty of obstetrician-gynecologist!) can be an x-ray technician.
- Dentistry is a dentist. We remember that the requirements refer to specialists with SECONDARY medical education. This means that a dentist can undergo appropriate training and become an x-ray technician.
- “Preventive dentistry” is a dental hygienist. He can also train to become an X-ray technician.
- “Orthopedic dentistry” is a dental TECHNICIAN. Yes, yes, that’s how fun it is in our country. A dental technician also has the right to receive the specialty “X-ray technician”, since he is a specialist with a SECONDARY MEDICAL education.
All of the above specialists have the right to undergo training (professional retraining) at a medical college and receive a certificate in the specialty “Radiology” and the position of “X-ray technician”. It’s funny - a dental technician can take pictures on his own, but a dentist cannot.
So, all of the above specialists, after undergoing professional retraining in the specialty “X-ray technician”, receive a certificate in “Radiology” and have the right to personally conduct X-ray examinations in the clinic.
Remember that to work as an X-ray technician, an employee must have two conditions at once: secondary medical education and a valid certificate in pre-medical radiology.
conclusions
A dentist does not have the right to perform x-ray examinations on his own; an assistant is required. This can be either a radiologist or an x-ray laboratory technician. He must be on the staff of the clinic and only he has the right to take pictures. If a dentist wants to perform x-ray examinations himself, he must complete a residency in radiology and receive the appropriate diploma and certificate.
How does a modern tomograph work?
The design of tomographs and the tomography technique itself have changed several times during the existence of the technology, replacing 4 generations.
The first tomographs had only 1 emitting tube and a detector moving around the object sequentially, layer by layer. Subsequently, an increased number of emitters and detectors was received.
The third generation introduced the concept of “spiral tomography”: an increased number of tubes and detectors in one step of the table synchronously carried out a full clockwise rotation, which significantly reduced the research time.
The fourth generation received a moving emitter (or several) and many rigidly mounted detectors on one ring. Now this is the most common type of tomograph, but third-generation devices are also available.
Modern tomograph
Accurate and fast analysis of organs is provided only by the latest generation devices with several emitters.
The most advanced modern tomographs operate on the fourth generation principle, but are equipped with a pair of radiation tubes mounted at an angle of 90 degrees relative to each other. They are exactly what is required to study organs in real time.
To examine soft tissues that merge with neighboring tissues on x-rays, contrast illumination is used - iodine-containing preparations that glow in the x-ray spectrum.
They are introduced into an organ or system, which then appear on a tomogram. For example, using an injection into a vein, you can highlight the circulatory system, and a drunk indicator reveals the gastrointestinal tract.
How harmful is it to have a CT scan?
Pay attention to the detail: the higher, the greater the radiation dose received
The procedure takes from 1 to 10 minutes, including when using the most modern devices. The longer, the greater the dose of x-ray radiation received by the body.
10 times higher than what is obtained with an x-ray : if doctors recommend doing it no more than 10 times a year, CT scans - 2-3 times.
Computed tomography of the lungs gives a dose of about 5 mSv (millisievert), of the abdominal cavity - 8 mSv, CT of the whole body - 10 mSv.
CT requires less personnel protection, but produces more radiation
On average, the radiation dose received during a single chest CT examination is 150 times higher than the dose received during a conventional X-ray. So you shouldn’t prescribe a CT scan yourself.
Living in central Russia, a person receives a radiation dose of about 3 mSv. An air flight from Moscow to Europe gives exposure to 0.05 mSv.
The maximum permissible annual dose of any ionizing radiation for a person is 100 mSv, and the resulting 250 mSv was guaranteed to send the liquidator home from the Chernobyl zone.
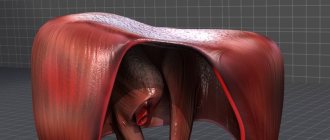
What is a diaphragm?
This is the muscle that separates the chest and abdominal cavity. A person needs it for breathing; it helps the pectoral muscles draw air into the lungs and expel it.
Diaphragm
The diaphragm also takes part in digestion, moving food through the esophagus. The muscle plays a great role in blood circulation; as it descends, it leads to an increase in internal pressure in the abdominal cavity, which provokes the “squeezing out” of blood from the liver into the lower vein, and then to the heart. Therefore, it is extremely important to have your diaphragm examined periodically to avoid health problems.
Who should not have a CT scan and when?
Children undergo CT scans only for serious illnesses
Tomography is strictly prohibited for pregnant women and is allowed only if necessary for children.
With “contrast” - iodine-containing drugs - there are much more restrictions.
In addition to those diseases for which it is expressly prohibited to take iodine-containing drugs, this type of examination is contraindicated for diabetics, persons with a body weight exceeding that allowed for the device, and patients in severe conditions, if the risk of the examination outweighs the benefit.
For everyone else, it can be done without fear - but only taking into account the total annual radiation dose, which should include flights, X-ray examinations and all other cases of interaction with ionizing radiation.
There are few of them in our lives, but they still exist.
When should you choose CT instead of X-ray?
X-rays in the form of flat images are simpler and safer for humans than a computer tomogram. However, the work of organs in real time cannot be seen on x-rays.
In the same way, x-rays are not able to show volumetric problems masked by other contrast inclusions, which often include tumors, problems with blood vessels, and complex injuries.
CT scans are also performed after operations, especially when metal prostheses, shunts or pacemakers are introduced
Therefore, CT scans are prescribed if an urgent decision is needed when serious problems of the heart and brain are suspected, as well as other emergency conditions, which include:
- head injuries accompanied by fainting,
- headache if there is a suspicion of serious disturbances in the functioning of the body,
- convulsions that appeared for the first time without a reason, and in combination with suspected systemic diseases,
- mental state disorders with suspected brain damage.
Routine and non-urgent CT examinations are carried out strictly as prescribed by the doctor in cases where simpler methods do not produce results. Otherwise, the radiation exposure is unreasonably high.
What does an x-ray show?
There are practically no clinical symptoms of problems with the diaphragm; in rare cases, the patient may complain of pain in the chest area. The onset of an abscess in a muscle is judged only by nearby internal organs. The main method for identifying problems with the diaphragm is radiography.
X-ray of the chest cavity
Initially, a survey x-ray of the chest cavity is performed in different projections. If there are diseases of the diaphragm in the image, the medical expert will be able to see the increased or decreased state of the dome, deformation, and the presence of malignant or benign tumors.
Some diseases are accompanied by complete or partial immobility of the diaphragm.
Hernias
They are formed as a result of prolonged high pressure inside the abdominal cavity, which can be caused by a prolonged and severe cough, or excess weight. A hiatal hernia on an X-ray is a rounded darkening; the disease is accompanied by symptoms such as heartburn and pain in the esophagus.
Diaphragmatic hernia
Most often in practice, a hiatal hernia occurs when part of the stomach ends up in the chest cavity. Sometimes the disease is accompanied by girdling pain, reminiscent of pancreatitis. A hiatal hernia can negatively affect the functioning of the heart and people begin to undergo treatment with a cardiologist for years without success, which is why it is always recommended to undergo a comprehensive examination.
It is important! To identify a hernia at an early stage, it is necessary to go for an X-ray of the esophageal opening of the diaphragm if there is any discomfort in this area. It’s better to play it safe than to undergo lengthy and unpleasant treatment later.
Inflammatory processes
Typically, an abscess begins as a result of gastrointestinal diseases such as ulcers, pancreatitis, appendicitis, and kidney problems. The main symptoms are fever and sweating, pain under the ribs, aggravated by coughing or sneezing. The patient suffers from shortness of breath and hiccups.
Diaphragm lesions
In some cases, a person is forced to constantly be in a semi-sitting position, since this reduces pain.
Relaxation
Characterized by thinning or complete absence of muscle mass of the diaphragm, the cause is a developmental deviation or pathology. It can be one-sided, accompanied by protrusion of the dome towards the chest cavity, or partial, with the dome bulging in a certain area.
Relaxation of the diaphragm is determined quite easily on an x-ray; the disease is diagnosed if the contour of the dome is located much higher than the required level; the stomach can be seen immediately below it. In lateral projection, the contour of the diaphragm together with the chest forms an acute angle. Most often, relaxation affects the left side.
Relaxation of the diaphragm on x-ray
Relaxation of the diaphragm on the right side on x-ray is much less common and is usually accompanied by interposition of the colon. The x-ray shows a significant difference in the height of the domes, and you can also see the intestine filled with gas.
Despite the opinion of some experts that x-rays are an outdated and uninformative method, the importance and value of this examination cannot be underestimated; for some diseases, this is the only way to diagnose the disease and get a complete picture of the patient’s health.